Participant perspectives on disability and therapeutic alliance revealed 4 major themes.
- Impact of disability, where participants elaborated on 4 sub-themes including: positive and negative impacts of being disabled, identity, and the impact of an acquired disability on self and family.
- Experiences with physical therapy, where participants shared both positive and negative experiences, as well as perceptions of goal achievement and progress.
- Perceptions of PTs with a disability, where participants described the perceived impact of a PT’s disclosure of their disability on therapeutic alliance and the overall physical therapy experience. They also distinguished physical and societal barriers faced by people with disabilities becoming PTs.
- Relationships, where participants identified sub-themes of shared identity and interactions.
Impact of Disability
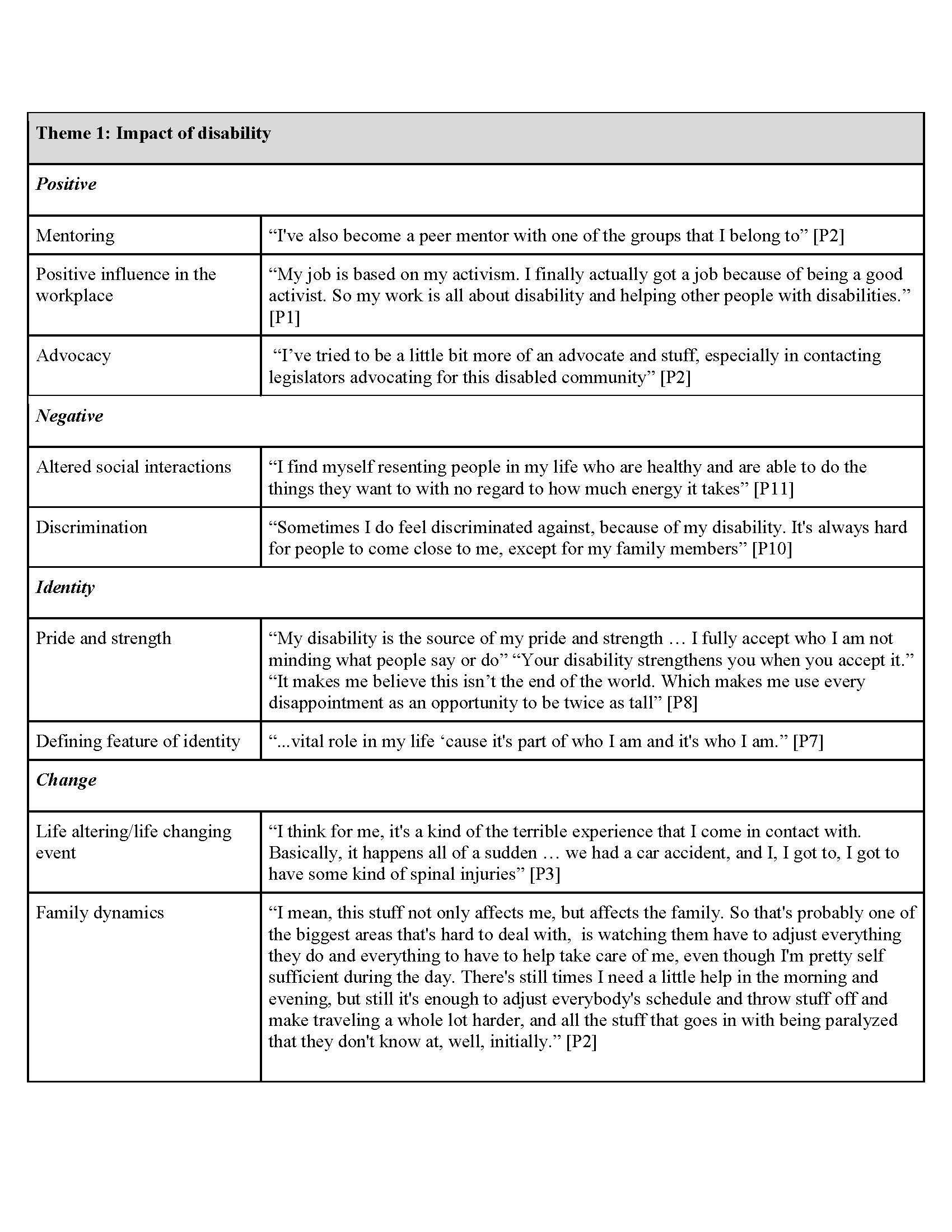
Participants shared mixed responses when asked about the impact of disability on their lives. Many expressed both positive and negative influences within their lives, as well as how their disabilities impacted their identities. Those who acquired their disability later in life also discussed the ways in which their disability changed their life. Thus, 4 sub-themes were identified: positive impact, negative impact, identity, and acquired disability impact.
Positive Impact. Positive aspects of disability were related to the experience of mentoring other individuals with disabilities, activism, and disability identity as a positive influence.
Negative Impact. All participants shared or agreed with examples of negative sequelae related to disability. Negative aspects of disability included discrimination and altered social interactions, which were detrimental to participants mentally and emotionally.
Identity. Some participants discussed the impact of disability on their personal identity. One participant shared that her disability had become a source of pride and strength. Others described their disability as a defining feature of their identity.
Acquired Disability Impact. Participants that acquired their disability later in life described their disability as a life-altering event and expressed feeling a change in their familial role and surrounding relationships.
Experiences with Physical Therapy
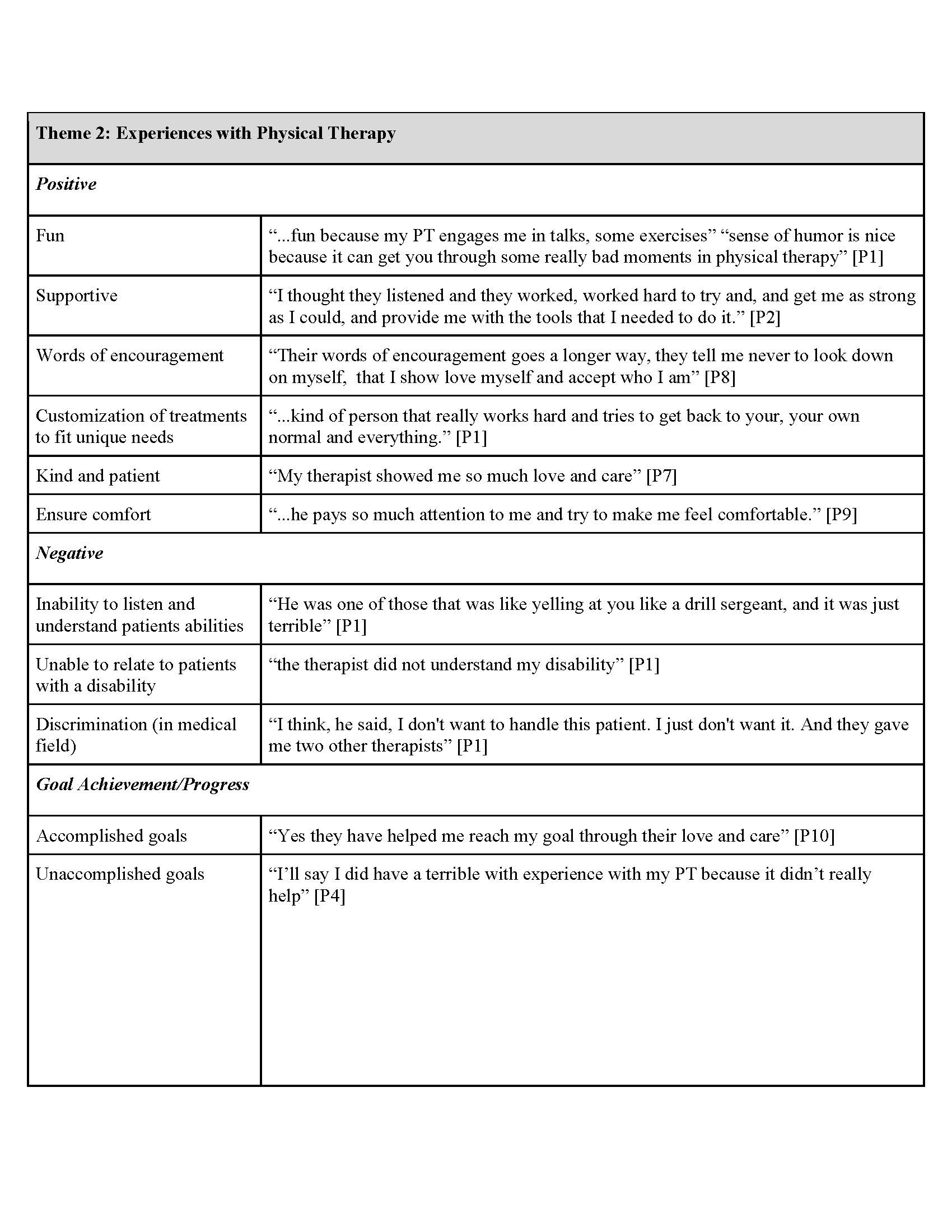
Experiences with physical therapy varied by individual, with participants sharing positive and negative experiences, and expressing their opinions regarding progress toward their goals throughout treatment. The 3 sub-themes identified were: positive experiences, negative experiences, and goal achievement and progress.
Positive Experiences. Positive experiences shared by participants included having fun while at physical therapy, receiving words of encouragement, and feeling supported throughout their treatment. Participants also described experiences where they felt their care plan was customized to fit their unique needs, and their PT was attentive, kind, patient, and made efforts to make them feel comfortable.
Negative Experiences. Participants described the inability of their PTs to listen and understand their abilities and experiences and felt that their non-disabled clinicians were unable to relate to IWDs. Some participants expressed feelings of discrimination in the medical field based on disability and race.
Goal Achievement and Progress. Most participants reported that positive experiences with physical therapy impacted goal achievement. Participants attributed the success of goal achievement to the genuine care clinicians demonstrated. Participants also described negative experiences during their healing process, including a lack of understanding from their PTs and unrealistic expectations being placed upon them, leading to unaccomplished goals.
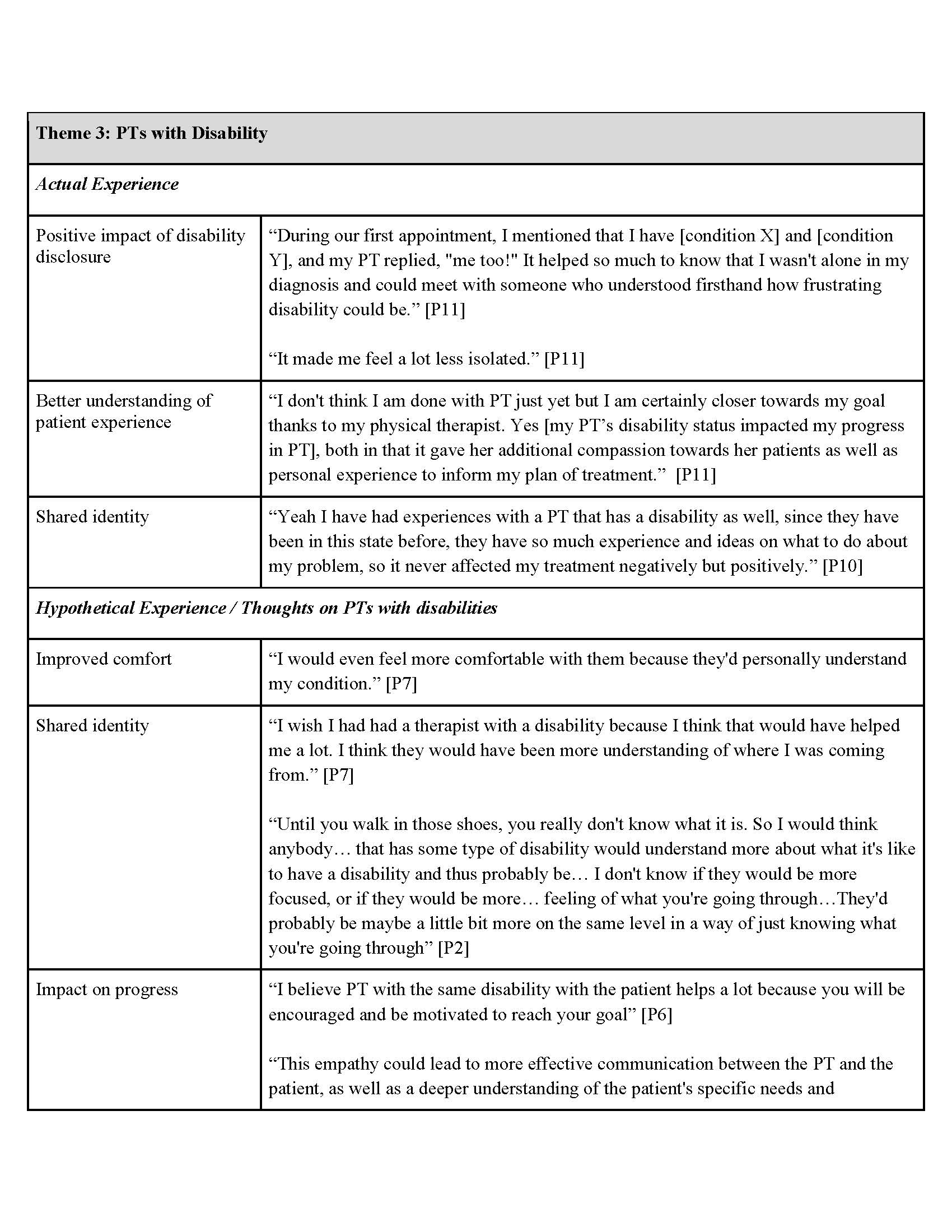
Perceptions of PTs With a Disability
Each group contained a mix of individuals who had been treated by a disabled PT and individuals who had not been treated by a disabled PT. Participants who were treated by a disabled PT discussed their experiences with treatment and their experiences with discussing their PT’s disability. Those who did not have a PT with a disability shared their thoughts on potentially being treated by a disabled PT. All participants expressed their thoughts on PTs with disabilities, as well as the positive impacts of people with disabilities becoming PTs. Two major sub-themes were identified: impact of experiences, and positive impacts. Discussion also touched on societal and physical barriers to PTs with disabilities.
Impact of Experiences. When treated by a PT who disclosed their disability, participants felt that this disclosure was a source of encouragement that helped with their recovery. They felt that their PT could better understand their experiences, and when seeking physical therapy care in the future, they reported only desiring to return to a PT with a disability. Participants treated by PTs who had the same disability as themselves felt more connected and validated due to shared circumstances; however, experiences with disabled PTs were overwhelmingly positive, regardless of differing diagnosis.
One participant who shared the same diagnosis as their PT commented:
“It helped so much to know that I wasn’t alone in my diagnosis and could meet with someone who understood firsthand how frustrating disability could be.”
Another participant stated that while they didn’t share the same disability with their PT, they felt that:
“…it gave her additional compassion towards her patients as well as personal experience to inform my plan of treatment.”
Participants treated by PTs that did not disclose a disability shared that they thought they may be more comfortable and open if treated by a PT with a disability. Some participants that were treated by non-disabled PTs expressed that non-disabled PTs can be competent in delivering high-quality care to disabled patients if they are skilled and attentive.
When asked to share thoughts regarding PTs with disabilities, participants expressed that shared disability status between a patient and clinician may be beneficial for treatment, and that clinicians that have both clinical and personal experience can positively impact patient progress in physical therapy. While shared disability status may be beneficial for treatment, one participant stated that everyone’s experience can differ greatly and that the disabled community should not be considered as a monolithic category.
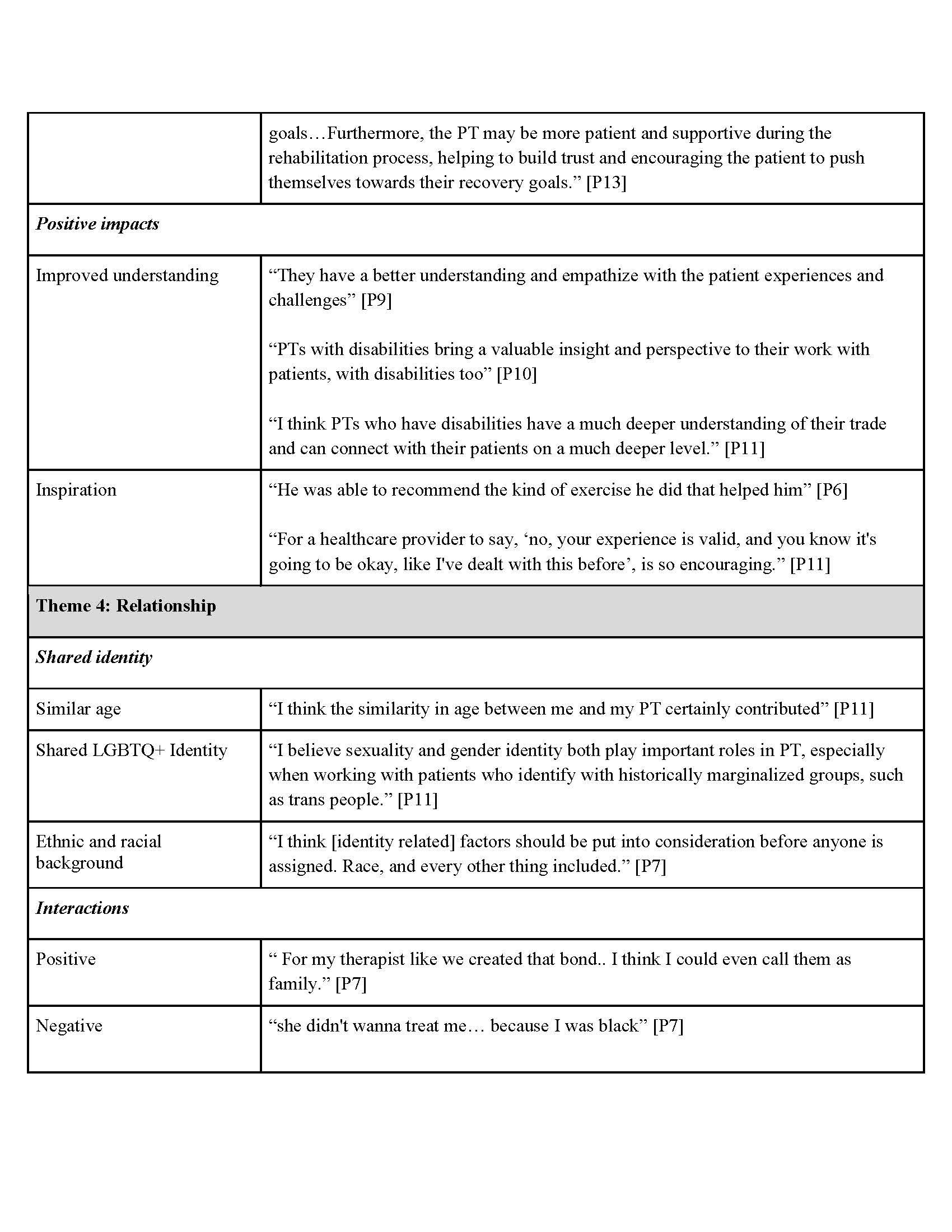
Positive Impacts. Participants felt that the lived experiences of having a disability would improve a PT’s understanding of disabled patients. Others, particularly those acquiring their disability later in life, described PTs with disabilities being a source of inspiration as they navigated mental health challenges surrounding their new disability. Participants also expressed that PTs with disabilities could be role models for others with disabilities, and one participant stated he was in the process of becoming a PT himself.
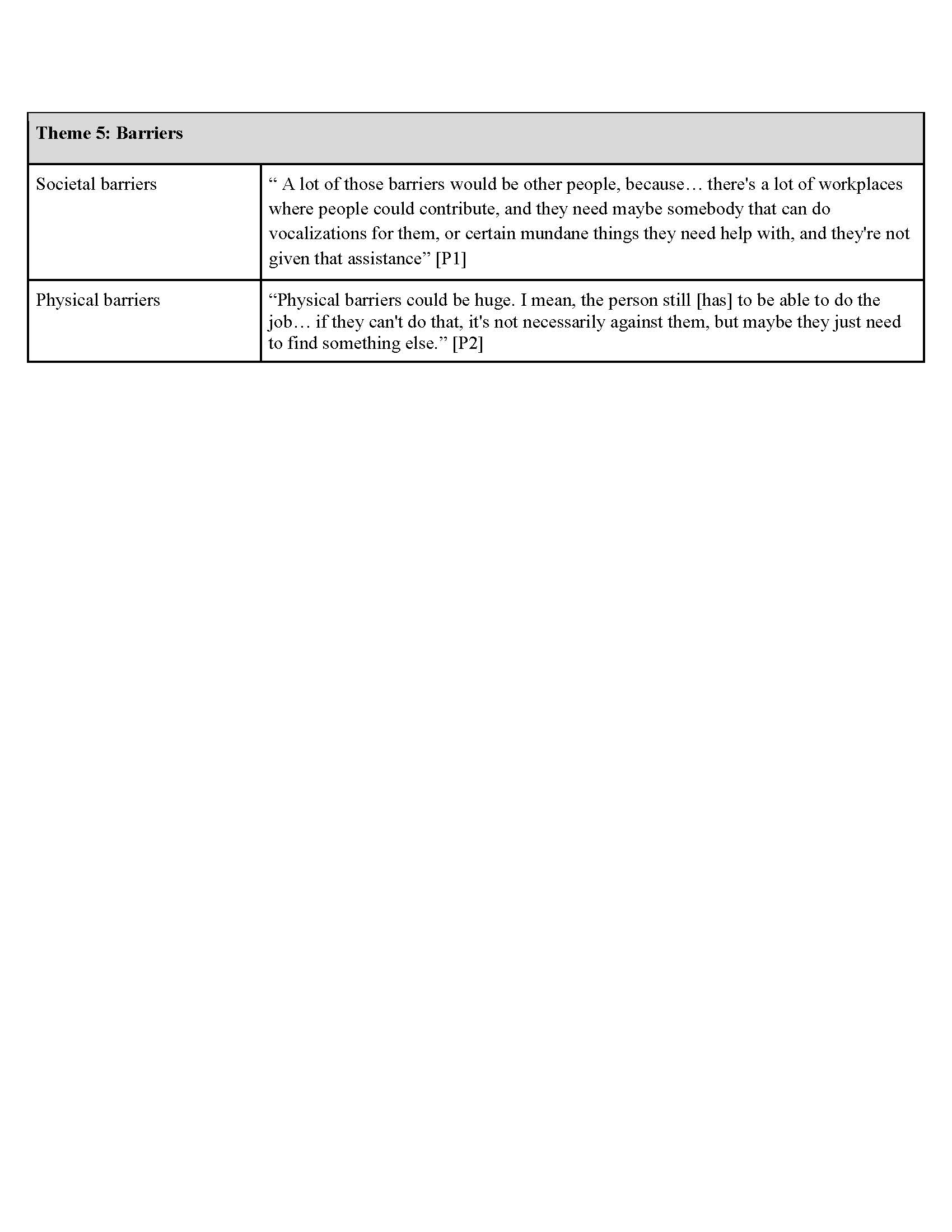
Societal and Physical Barriers. Some participants discussed the barriers that people with disabilities face in becoming PTs. Barriers included societal barriers, such as discrimination and lack of necessary accommodation, and physical barriers, such as physically-demanding job tasks.
Factors Impacting TA Relationships
Various qualities, attributes and interactions contributed to the relationship that participants had with their PTs. Two sub-themes were identified as contributing to a positive relationship between patients and clinicians: shared identity, and impact of interactions.
Shared Identity. Participants expressed that having something in common with their PT fostered a stronger relationship. This included being of similar ethnic or racial background, having a shared LGBTQ+ identity, or being similar in age.
Impact of Interactions. While sharing their physical therapy experiences, participants often discussed the interactions that they had with their PTs and the role the PTs played in shaping their experience. Negative experiences involved interactions where participants felt discriminated against or misunderstood by their PT. In contrast, interactions leading to positive experiences included feeling welcomed and being treated with compassion, similar to how one would treat a family member.
Discussion
The present study explored the perceptions and experiences among IWDs regarding TA within physical therapy. Discussions revealed multiple potential impacts on this relationship, including shared identity.
Importance of Shared Identities
While this study did not categorize the specific disabilities of the PTs involved, participants noted that the disclosure of disability by a provider, regardless of the specific diagnosis, was the primary catalyst for an improved therapeutic alliance. This suggests that the shared social identity of being disabled may be more significant to the alliance than clinical diagnostic concordance. Participants that shared positive experiences with physical therapy treatment emphasized the importance of empathy and understanding and expressed feeling more comfortable when their clinician was able to validate their experiences. Some participants appreciated it when their PTs had a sense of humor, which made their sessions more enjoyable. A variety of shared identities, through similar age or interests, were perceived to improve TA.
These findings extend to recent research regarding the positive impact of TA-based treatment approaches as evidenced by improvement in pain intensity via pain assessment scales (VAS PI-NRS) for treatment of chronic low back pain.12 The current findings highlight contextual factors that may impact the magnitude of treatment effects for physical therapy interventions.
Negative Experiences
Some participants reported negative experiences with physical therapy, notably citing incidents in which the PT did not demonstrate consideration for the individual’s experience. Lack of consideration may be attributed to aversive ableism—for instance, when a well-intentioned clinician unknowingly engages in implicitly biased thoughts or actions.7,8,11 Research has identified that healthcare workers often lack the knowledge, skills, and confidence to care for people with disabilities, with discriminatory attitudes and behaviors being widespread across all healthcare services and income levels.26
Thus, it is important for non-disabled clinicians to understand the construct and experience of disability. Developing this understanding improves care by shifting the clinical lens from a biomedical focus on ‘normalizing’ function to a partnership that prioritizes the patient’s autonomy and quality of life. To achieve this, physical therapy education must go beyond the ICF model to integrate principles from disability studies and the humanities, exposing students to the social and political dimensions of disability.
Mitigating Aversive Ableism
Additionally, clinicians can work to mitigate aversive ableism by seeking meaningful contact with individuals with disabilities outside of clinical settings, such as through community engagement or advocacy groups, which has been shown to reduce implicit bias more effectively than didactic training alone.10 By valuing the lived experience of disability as a legitimate form of evidence alongside clinical expertise, non-disabled PTs can build a more authentic therapeutic alliance that validates the patient’s identity rather than seeking to ‘fix’ it.
A New Perspective on Identity. Throughout the focus groups, the topic of identity was a recurring theme. Although some participants—especially those with an acquired rather than congenital disability—viewed their disability as a barrier, most participants viewed their disability as a source of pride or a defining characteristic in their identity. Historically, the profession of physical therapy has emphasized maximizing patient independence by limiting disability.27 However, implying that an individual’s disability is something that needs to be intervened upon to align with a non-disabled “norm” is inherently ableist and could negatively impact TA.11 This sentiment was shared by participants as they discussed feeling that providers framed their disability as something to be “fixed,” which contributed to a poor patient-provider relationship.
The Concept of Social Constructs. To address this phenomenon, incorporating the conceptualization of disability as a social construct through narrative means may be beneficial for clinicians working with IWDs to improve their ability to connect with this population.28 For example, neurodiversity approaches emphasize that both the individual and the environment factor into the construct of disability and assert that all minds and brains should be accepted and valued—not labeled with negative judgment.29 Following this principle, interventions within the context of disability in healthcare are to facilitate adaptations, through new skills and/or adjustments in the environment to promote improved quality of life determined by the patient. By protecting self-autonomy through empathy and respect, both patient-provider relationships and health outcomes may be enhanced.
Provider-Patient Concordance
Regarding identity, the importance of provider-patient concordance in healthcare has been well-established in other research domains. Research on racial and ethnic concordance has suggested that it can positively enhance communication and patients’ healthcare experiences, participation in clinical decision-making, intentions to adhere to clinicians’ recommendations, and satisfaction with care.30 Further, social concordance has been shown to predict differences in medical visit communication and patients’ perceptions of care, with lower concordance associated with less positive patient perceptions and lower positive patient affect.16
These findings suggest that concordance across various identity dimensions can impact healthcare quality and patient experiences. PTs who identify as having a disability may be in a position to connect with the experiences of their patients. Given that a clinician’s personal experience of disability may lead to an increased understanding of the experiences and goals of patients with disabilities,31 it follows that the shared identity of disability between clinicians and patients has the potential to improve patient health outcomes.
Furthermore, if a disabled clinician discloses their own disability to a disabled patient, our data suggests that the patient may feel safer with this clinician due to their shared identity, regardless of disability type. This increased sense of safety and trust may then lead to increased therapeutic alliance, which has been shown to positively impact treatment outcomes.
When PTs treating the focus-group participants disclosed their disability, participants recalled feeling encouraged and believed it improved their recovery. Additionally, many of those who had the experience of being treated by a PT with a disability expressed that they preferred this experience and would seek it out in the future. Likewise, many of the focus-group participants, whether having been treated by a PT with a disability or not, expressed a desire for greater diversity within the physical therapy profession.
Barriers to IWDs Becoming PTs
While shared identity between a patient and a provider can improve TA and healthcare outcomes for IWDs, numerous barriers exist for IWDs becoming PTs. Such barriers interact at and between the cultural, institutional, interpersonal, and intrapersonal levels of society. At the cultural and interpersonal levels, there is: stigma, abuse, harassment, and skepticism surrounding one’s capabilities and clinical skills.17 These discriminatory forces have continued to gain traction in the current political climate in the US, where federally-funded Diversity, Equity, and Inclusion (DEI) programs are being stripped of their value, demoralizing all who benefit from those initiatives.26,32
At the intrapersonal level, there is internalized ableism, where IWDs may internalize societal messages about their worth and capabilities. At the institutional level, in academic programs and clinical settings, ableist technical standards and/or essential functions dictate the physical, behavioral, or cognitive abilities required.33 These requirements often focus on how an individual completes a task (eg, seeing, hearing, walking, lifting), rather than the overall ability to achieve a task. As a result, PTs and student PTs may be hesitant to disclose their disability to their employer or program, in fear of being perceived as less competent.
Despite the implications of these requirements, PTs with disabilities can be capable clinicians when provided proper accommodation. Excluding IWDs from joining the profession ultimately dampens the diversity of the workforce and allows for continued cultural, institutional, interpersonal and intrapersonal perpetuation of stigma and bias due to a lack of peer relationships, knowledge, and critical awareness of disability.
Notably, technical standards are not required by any governing bodies of the physical therapy profession. The Standards of Practice for Physical Therapy as outlined by the American Physical Therapy Association cite patient and client management practices as being based in evidence-based practice through the 3 core components of clinical expertise; best available research evidence; and patient values, preferences, expectations, and context. None of the standards outlined specify the method in which the performance of clinical responsibilities should be completed, rather focusing on the outcomes that must be obtained for competent provision of physical therapy services.34
Further, first-person narratives from disabled clinicians and students, such as those emerging from the ACAPT Advancing Accessibility and Disability Equity Summit, offer powerful testimonies to the value of shared identity in fostering community, empowerment, and optimism within the profession.35 These narratives demonstrate that through art, literature, and storytelling the humanities are essential tools for understanding the human experience of disability, and for cultivating the deep humanistic relationships that underpin effective rehabilitation practice.
Limitations
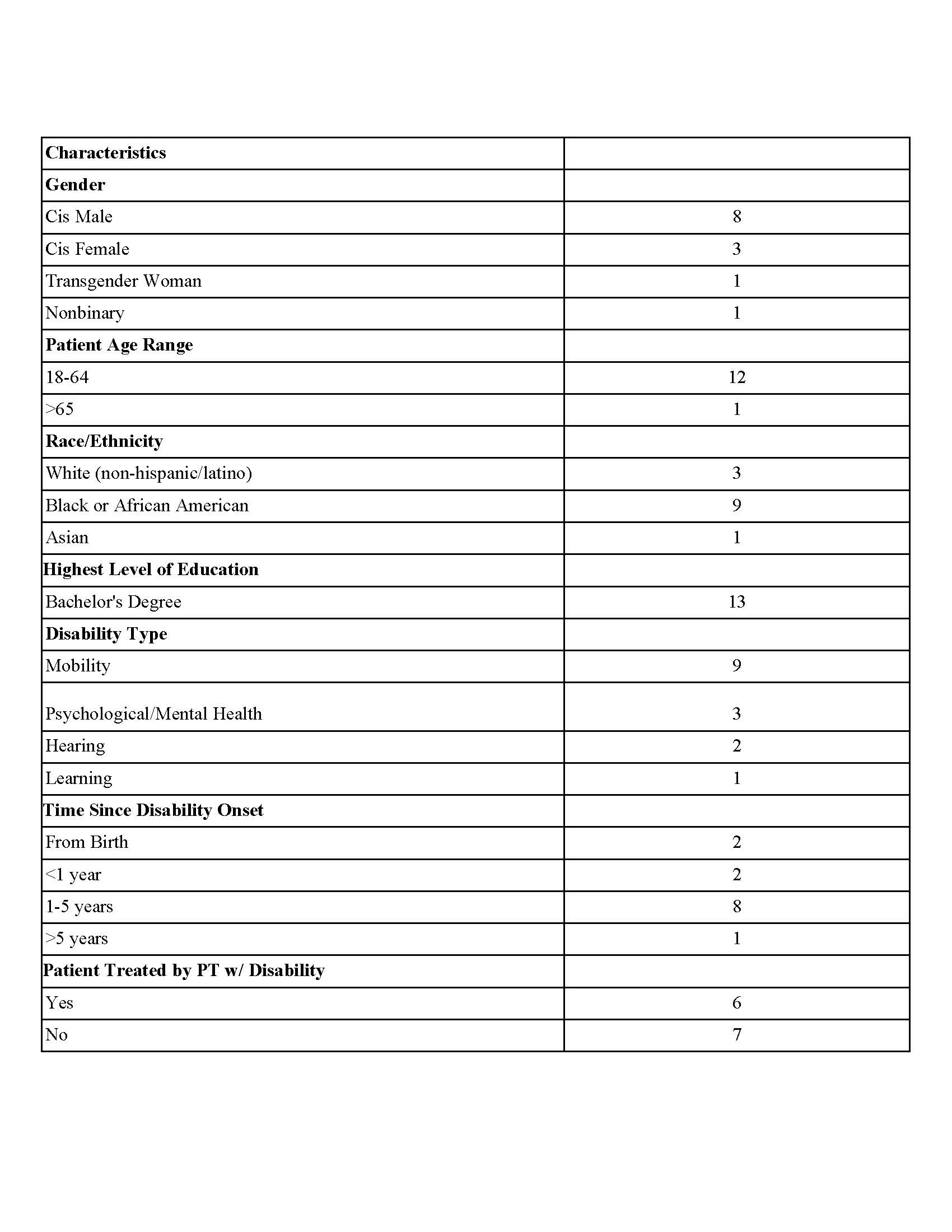
There are several limitations to the current study. The recruitment area included the entire US, which led to limited availability of focus-group time slots due to differing time zones. Additionally, due to these time-zone and geographic differences, focus-group meetings were conducted via Zoom. Initially, 21 participants were selected and scheduled for the focus groups. Many participants were dropped from the study due to reasons such as connection issues, failure to sign the consent form, and refusal to participate due to lack of financial compensation. A total of 13 participants remained and were included in data analysis. Due to participant drop-out, participants were not uniformly distributed across the 3 groups and data from each group varied greatly. Group 1 was the strongest for thematic analysis, with all participants making contributions to the discussion. In groups 2 and 3, some participants answered more questions than others, and the “chat” feature was heavily utilized instead of participation in verbal discussion, which limited the ability of participants to converse with one another. The small sample size and varied participation from focus-group members limit the generalizability of this study.
Conclusion
This study examined the impact of IWDs being treated by a PT with a disability on TA to better understand the potential influence of this shared identity on their experience with physical therapy.
Participants with disabilities indicated overall positive perceptions of, and experiences with, PTs with disabilities, and a potentially positive impact on TA.
These findings can inform the physical therapy profession, as several barriers to IWDs becoming PTs exist and the profession would benefit from diversification in students and clinicians alike.
Simultaneously, the profession must commit to anti-ableist training for all clinicians, ensuring that the burden of education does not fall solely on providers with disabilities.