Introduction
Doctor of Physical Therapy (DPT) programs should equip students with the knowledge and clinical skills to satisfy contemporary practice demands and individualized, holistic patient care. The Commission on Accreditation in Physical Therapy Education ensures DPT programs meet certain curricular requirements, including diverse clinical education experiences (CEEs).1 The affective, cognitive, and psychomotor learning domains are core tenets of assessment tools commonly used to assess student performance during their CEEs.2,3 Poor communication and unprofessional behavior have negative impacts on student clinical performance.4,5 Although difficulties across all domains contribute to DPT student clinical education challenges, one study found that the affective domain is the most common area of student struggles.5 However, DPT education historically emphasized cognitive and psychomotor domains. 6
The Affective Domain of Learning
The affective domain of learning includes interpersonal skills, resilience, self-reflection, ethical awareness, and compassion needed to foster an effective therapeutic alliance between physical therapists and their patients and patient families. A strong therapeutic alliance is associated with higher patient satisfaction, better outcomes, and improved quality of life.7,8
The Compassionate H.E.A.R.T Model. Several therapeutic alliance frameworks related to physical and occupational therapy exist.7 The Compassionate H.E.A.R.T. (Helping Ease, Alleviate, & Relieve Therapeutically) model9 is a modernized approach honoring the complexity of human experience in healthcare, and offering students and clinicians a framework to navigate the patient-provider interaction. Although the model incorporates cognitive and psychomotor domain skills, it is rooted in affective abilities essential for holistic patient care, with communication, empathy, and emotional intelligence (EI) as core tenets.
The Compassionate H.E.A.R.T model recognizes both the objective and subjective aspects of patient vulnerability, encouraging providers to engage authentically and empathically with patients’ lived experiences.9 Central to this engagement is communicating verbally and nonverbally through active listening, tailored language, and compassionate presence.
Communication. As a dynamic and reciprocal process, communication is foundational for building trust and forming therapeutic bonds. Nonverbal cues, including eye contact, body language, and tone of voice, reinforce respect and emotional safety, helping patients feel seen and understood.10,11 However, concerns exist about inadequate communication training in physical therapist education.12 Despite more recent emphasis on the affective domain, communication skill development is needed to ensure the long-term success and sustainability of the profession.13
Empathy. The therapist’s intention to remain within the patient’s frame of reference and understand their feelings (empathy) is deeply intertwined with communication.14 Empathic providers are more likely to engage in patient-centered care and foster shared decision-making, improving satisfaction, adherence, and diagnostic accuracy.14,15 However, empathy is not a static construct; DPT students’ empathy often declines throughout their education and improves only as they enter practice, highlighting the need for intentional cultivation.16,17
Emotional Intelligence is an essential competency in healthcare, enabling providers to recognize, understand, and manage emotions in themselves and others.18,19 High EI enhances patient-provider interactions and is linked to better clinical outcomes and greater patient and practitioner satisfaction levels.20-22 Despite its importance, DPT curricula often rely on CEEs to develop EI, yet studies show that validated EI measures do not significantly improve throughout education.22-24
Structured training within DPT programs can improve the interpersonal skills and support the development of holistic, emotionally attuned clinicians.25 Targeted workshops, lectures, group discussions, and role-playing have improved empathic interactions in nursing,26 pharmacy,27 and physical therapy students,28 with longer training programs resulting in superior outcomes. These efforts are often included in coursework without a direct connection. Outcome studies are conflicting regarding the short- and long-term effectiveness of these structured programs,27-30 and studies frequently lack control groups, limiting the ability to draw causal conclusions.28,30 Furthermore, the overlapping and inconsistent use of constructs such as communication, empathy, and EI creates challenges for healthcare research, education, and assessment.9
Purpose of This Study
Therefore, this study’s primary aim was to evaluate changes in communication, empathy, and EI following participation in a structured distance-based instructional program concurrent with second-year DPT students’ intermediate CEE. Two secondary aims were to:
- Examine the extent to which these affective competencies relate to one another.
- Qualitatively explore students’ perceptions, attitudes, and reflections about their experiences with the instructional program.
It was hypothesized that participation in the training program would lead to measurable improvements in communication, empathy, and EI, and that these skills would show positive correlations with one another.
Materials and Methods
A quasi-experimental repeated-measures design examined the impact of a distance-learning training program on second-year DPT students during their 8-week intermediate level CEE. Participants were recruited through emails provided by Program Directors from two DPT programs in the Northeastern United States. The experimental group consisted of a convenience sample of two consecutive cohorts of second-year DPT students (Cohort A and Cohort B) from the program where the primary and secondary authors serve as Directors of Clinical Education (DCEs).
These students took part in a modified version of the Level-Up Initiative (LUI), an established distance-learning curriculum designed to bridge gaps in interpersonal skills training within DPT education. The control group, consisting of two consecutive cohorts of second-year DPT students from another DPT program of similar size and clinical education structure, completed their standard intermediate-level CEE without receiving any additional formal instruction related to communication, empathy, or EI. Students holding a prior license in a health-related field were excluded from both groups.
Survey Administration
All participants completed the same survey at two time points. Both the control and experimental groups completed the baseline survey after finishing their second year of didactic coursework, before beginning their intermediate-level CEE. The control group completed a follow-up survey within one month of finishing the CEE, while the experimental group completed the same survey within one month of finishing the LUI training program. For both groups, follow-up survey completion occurred before the start of the third-year didactic coursework. Only fully completed surveys were included in the final analysis. Although the LUI was a required component of the experimental group’s institutional CEE curriculum, participation in the research study was voluntary and anonymous. The study protocol was approved by the Institutional Review Board at the New York Institute of Technology.
Survey data was collected and managed using a secure electronic data capture tool (REDCap).31,32 Survey access was granted after selecting “I consent” to the question, indicating their informed consent to participate. No identifying information was collected from any of the participants. The survey included 3 validated self-reported survey instruments (Appendix A).
- The Jefferson Scale of Empathy (JSE) is a widely utilized tool for measuring empathy among healthcare professionals with good reliability and construct validity.30,33 The survey consists of 20 items scored on a 7-point Likert scale, with scores ranging from 20 to 140, with higher scores reflecting higher levels of empathy.
- The Schutte Self-Report Emotional Intelligence Test (SSEIT)24 has good internal consistency, test-retest reliability, and construct and criterion validities.24,34 The 33-item instrument includes subscales for emotion perception, use of emotions, and management of self-relevant and others’ emotions. Items are rated on a 5-point Likert scale, with higher scores indicating higher EI levels.
- The Self-Efficacy Questionnaire-12 (SE-12) is a reliable and valid 12-item questionnaire designed to evaluate clinical communication skills. 35 The instrument is scored on a 10-point Likert scale, with scores ranging from 10 to 120, with higher scores reflecting more developed communication skills. The instrument has strong internal consistency with a Cronbach’s α of 0.95, and acceptable test-retest reliability with an intraclass correlation coefficient agreement of 0.71 (0.66–0.76).36
Focus Groups
After completing the LUI program, all participants from the experimental group were invited to participate in a focus group of no more than five students. Although recommendations suggest focus groups contain 6 to 12 participants,37 the authors chose to limit each group to five to ensure that all participants felt comfortable expressing their views without being discouraged or pressured, given their familiarity with one another. If more students volunteered, additional focus groups were formed. Informed consent was obtained from each participant verbally at the start of each focus group. An experienced qualitative researcher (JG) not associated with the students’ academic programs conducted semi-structured focus groups via videoconferencing (Zoom® Communications, Inc., San Jose, CA, USA), querying participants on their experiences with the LUI curriculum (Appendix B). Participants were de-identified to maintain confidentiality and integrity. Focus groups lasted approximately 45 minutes and were recorded and transcribed.
The Level-Up Initiative Training Intervention
The mission of the LUI is “to transform people to transform healthcare.” This program was designed to advance the professional development of students and practitioners in the rehabilitation and wellness fields, expanding on the interpersonal skills and critical thinking instilled during entry-level education. The program’s remote formats accommodate the diverse geographic locations, schedules, and settings typical of DPT clinical education experiences, supporting the feasibility of implementation and the generalizability of its use across varied contexts. Instruction was coordinated by the LUI founders, reducing potential bias from faculty and DCEs.
While the LUI program is grounded through an orthopedic physical therapy perspective, the content is transferable across diverse practice settings and clinical specializations. Since its creation in 2018, the LUI program has trained over 2,000 DPT students, early-career physical therapists, and other rehabilitation professionals practicing in a variety of settings; however, evidence regarding its effectiveness with these groups is lacking.
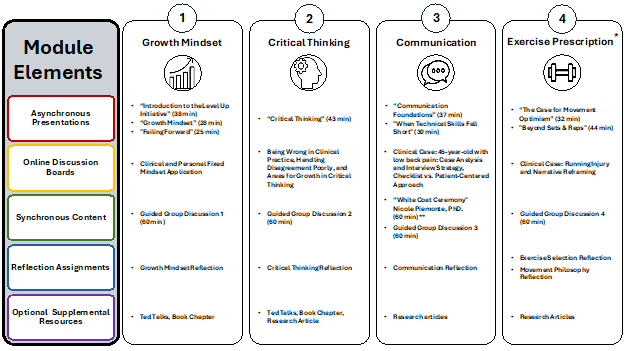
The program consisted of four monthly modules combining asynchronous content, synchronous group discussion, and written self-reflection (Figure 1). Participants progressed through monthly modules at their own pace, requiring approximately two hours to view content, complete reflection entries, and engage in guided group discussions. The experimental group’s DPT curriculum includes a 4-month interval between the second- and third-year didactic coursework, during which the students complete their 8-week intermediate-level CEE. To accommodate students’ varying CEE dates, the LUI curriculum was offered in two sections, ensuring all students completed the full program, with some content occurring outside of their CEE. Due to variations in students’ CEE start dates, the specific overlap between the CEE and the LUI program varied for each participant.
- The first module, Growth Mindset, focused on enhancing empathy, humility, and EI by fostering self-awareness, openness to feedback, and a deeper understanding of patients’ experiences and potential for change.
- The Critical Thinking module emphasized the application of a biopsychosocial, holistic, and patient-centered care approach, and the flexibility in updating beliefs based on evolving evidence.
- The Communication module centered on developing verbal and non-verbal skills to support compassionate and empathic patient interactions and therapeutic alliance building.
- Lastly, the Exercise module integrated concepts from previous modules to guide the prescriptions of patient-centered exercise programs through a biopsychosocial lens.
After the program’s first year, the DCEs reviewed course evaluations from Cohort A and shared this information with the LUI coordinators. In response, Cohort B’s training program was revised the following year by removing the Exercise module and expanding the Communication with additional synchronous content, ensuring consistency in total contact hours across cohorts.
The LUI asynchronous program was delivered by the program’s founders, with slight adaptations from the original design to align with the intervention group’s CEE schedules. An online community-building platform (Circle©) facilitated curricular organization, resource sharing, and communications. The synchronous group discussions were conducted over the Zoom® web-based video conferencing platform and consisted of one instructor and 4 to 7 students.
Licensed physical therapists who had previously completed the LUI program facilitated the guided group discussions. These clinicians, selected by the LUI founders for their extensive experience and ability to apply LUI concepts across diverse settings (e.g., outpatient orthopedics, outpatient neurology, inpatient rehabilitation), had no prior relationship with participants. Despite efforts to cluster students by CEE settings and match them with instructors of similar clinical expertise, schedule inconsistencies made it challenging to form homogeneous learning groups. Although the facilitators received no formalized training, a planning meeting was held by the LIU founders, and written instructions were provided to help maintain instructor consistency.
Data Analysis
Statistical analysis was conducted using SPSS (Version 24). Although the LUI program was modified between Cohorts A and B, preliminary analyses indicated no significant differences in demographics or outcome measure scores (JSE total score, p=0.954; SSEIT total score, p=0.987; SE-12 total score, p=0.451), and the cohorts were collapsed into a single experimental group for analysis. Demographic differences in age between the experimental and control groups were assessed using an independent t-test. Chi-squared tests analyzed group differences in sex, initial CEE clinical setting, and intermediate CEE clinical setting.
Due to the non-normal distribution of the data and the ordinal nature of all outcome measures, non-parametric statistics were utilized. Two-tailed Wilcoxon signed-rank tests evaluated changes in JSE, SSEIT, and SE-12 total scores before and after the students’ CEE completion. An alpha level of 0.05 was set for statistical significance. Effect sizes (r) were calculated by dividing the Z standardized test statistic by the square root of the sample size. Spearman’s Rank Correlation Coefficient identified relationships between JSE, SSEIT, and SE-12 scale scores. The Circle© platform evaluated each student’s progress within the LUI program completion to quantify program adherence.
Inductive content analysis was used to identify focus group themes. This approach allows categories and patterns to emerge directly from the data, as prior evidence regarding affective training interventions delivered during CEE in physical therapy education is limited.38 NVivo Software (QRS International, Version 1.7.2) was used to organize, code, and analyze qualitative data. Two researchers, with research doctorate degrees and experience with qualitative research analysis, independently coded the transcripts. Several consensus coding meetings were employed to enhance trustworthiness and inter-rater reliability.
Codes were first grouped into categories based on similarity and overlap, refined through discussion to capture broader patterns, and synthesized into overarching themes that represented the central ideas and experiences expressed by participants. This process incorporated self-reflection and bracketing, allowing researchers to set aside personal biases and minimize the influence of prior assumptions.
To establish credibility and confirmation of the findings, an independent, experienced qualitative researcher (JG) not associated with study participants or the academic program reviewed the de-identified transcripts, themes, and representative quotes, resulting in a collapsing of two initial themes and minor edits to theme descriptions and exemplar selections.38 Further credibility was established through member check verifications of final themes, descriptions, and representative quotes. Integrating these strategies helped investigators ensure that findings accurately reflected participants’ experiences.
The researchers acknowledge their dual roles as both investigators and as the participants’ DCEs. While this positionality provided valuable insight into the context of clinical education, it also carried the potential for perceived coercion or power imbalance. To mitigate these risks, several safeguards were implemented.
- First, although the LUI program was required as part of the students’ intermediate CEE, participation in the study was separate and optional, ensuring students retained autonomy over their involvement.
- Second, anonymity was maintained throughout to reduce the influence of social desirability bias and to protect participants’ confidentiality.
- Finally, focus group participation was voluntary, and informed consent emphasized that choosing not to participate would have no impact on students’ academic standing.
Results
Eighty-six DPT students were included in the final analyses. The experimental group included 56 students (100% response rate) with a mean age of 25.5 ± 3.3 years and demonstrated a combined 73.3% LUI program adherence. Sixty-six students were recruited for the control group, resulting in 47 responses. After data organization and cleaning, 17 participants had incomplete data and were excluded. Therefore, the control group comprised 30 students (45.5% response rate) with a mean age of 28.8 ± 3.8 years.
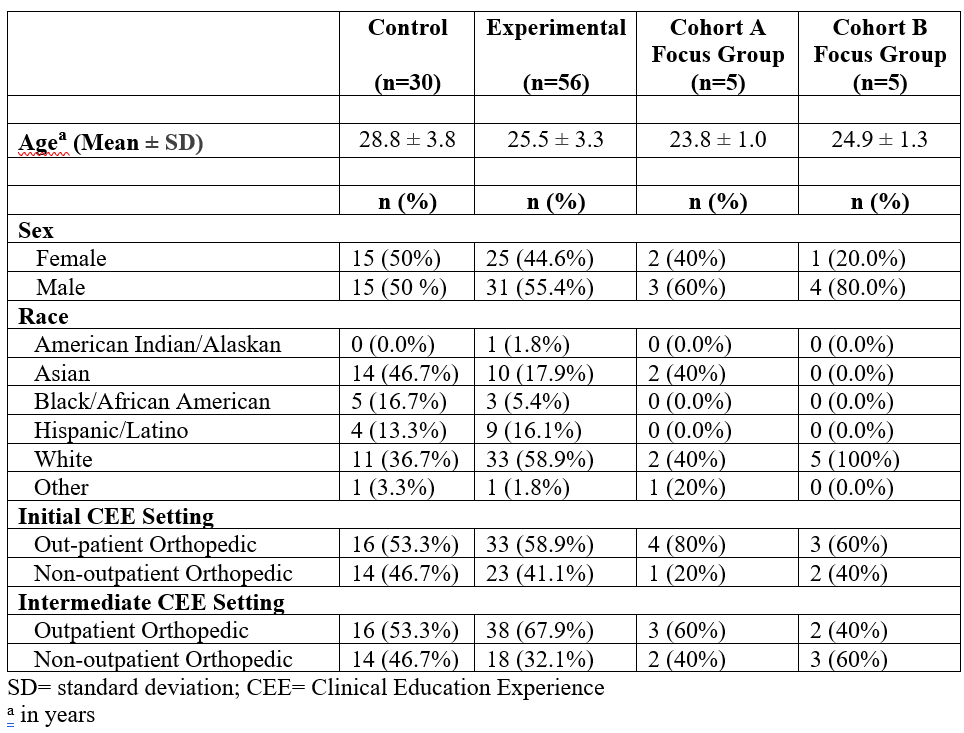
The demographics of the study and focus group participants are outlined in Table 1. There was a significant difference in age between the experimental and control groups (t = 4.161, p < .001), but no differences in sex (X2=.225, p = .634), initial CEE setting (X2=.249, p = .617), or intermediate CEE setting (X2=1.763, p = .184).
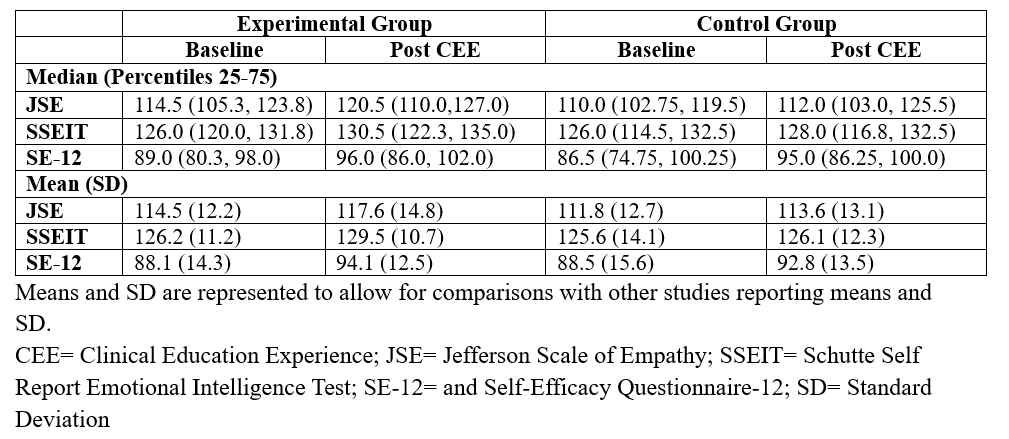
Descriptive statistics for JSE, SSEIT, and SE-12 scores for the control and experimental groups are presented in Table 2. The experimental group demonstrated statistically significant improvements across all outcome measures: JSE: Z = -3.51, p < .001, r = .47 (moderate effect); SSEIT: Z = -2.93, p = .003, r = .39 (moderate effect); and SE-12: Z = -3.19, p = .001, r = .43 (moderate effect).
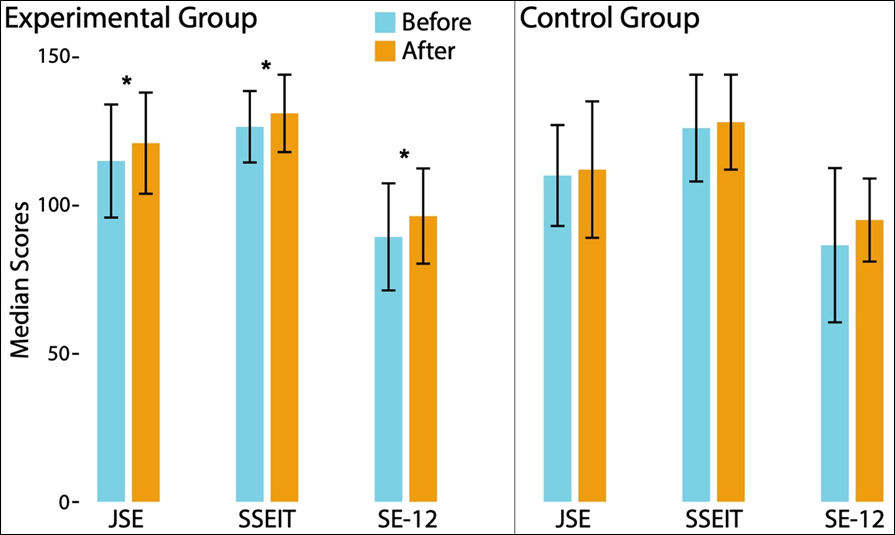
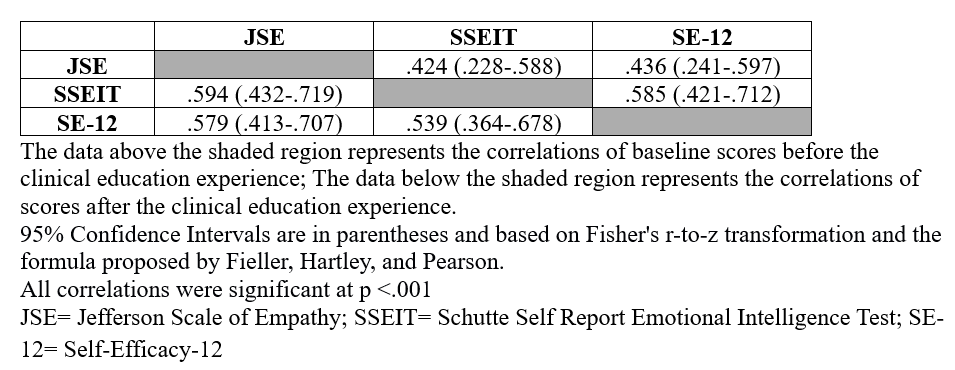
In contrast, no significant changes were observed in the control group: JSE, Z = -1.30, p = .194; SSEIT, Z = -.75, p = .455; SE-12, Z = -1.52, p = .128 (Figure 2). Significant positive, moderate correlations (rs=0.424 – 0.594, p < .001) were found between JSE, SSEIT, and SE-12 scale scores across the sample at baseline and after CEE completion (Table 3).
Focus groups included 5 students from each experimental cohort, yielding a total of 10 participants (17.8% of the sample). Because focus group participation was voluntary, the small number of participants could not ensure data saturation.
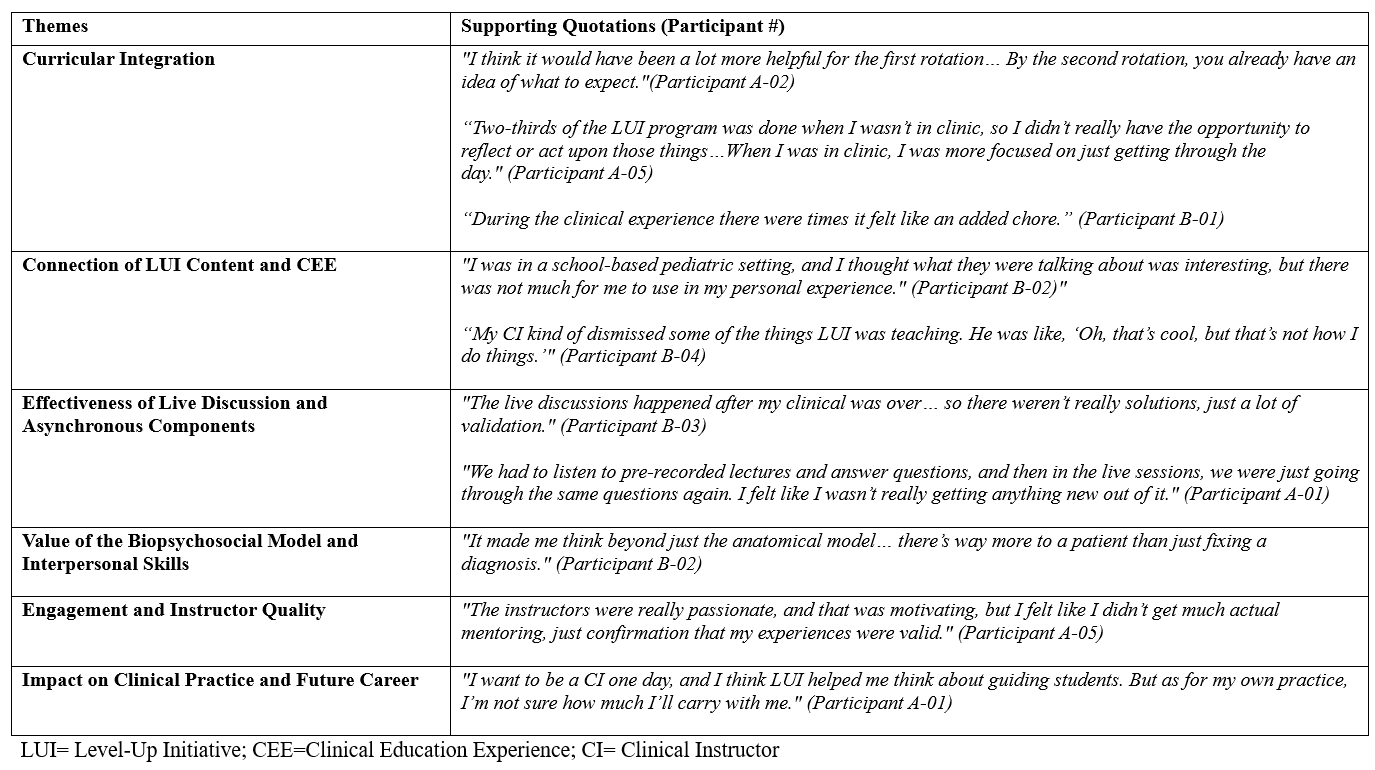
Thematic analysis revealed six key themes regarding students’ experiences with the LUI curriculum. Supporting quotations for each theme are provided in Table 4. All member checks (90% response rate) verified the accuracy of the themes and supporting quotations.
Theme One: Curricular Integration
Students expressed their feelings on how the LUI program was positioned within the DPT curriculum. Students commonly questioned the timing of its delivery, suggesting it might be more appropriate earlier in their training or offered as a post-professional continuing education course. Many reported difficulties balancing the program’s time demands with their CEE and often viewed it as an additional burden rather than an integrated or enriching component of their learning experience.
Theme Two: Connection of LUI Content and CEE
Students shared their perceptions of the LUI program content and its application during clinical education, particularly how the skills translated into real-world clinical environments. Many students noted challenges in applying concepts in certain settings, such as acute care, where contextual demands differed from those emphasized in the program. Some reported that clinical instructors did not fully align with LUI principles, further limiting opportunities to integrate and practice these skills during rotations.
Theme Three: Effectiveness of Live Discussion and Asynchronous Components
Students discussed the curriculum’s instructional formats, particularly the synchronous discussions and asynchronous content. Students generally valued the synchronous discussions for providing meaningful interaction, deeper reflection, and opportunities to learn from their classmates’ experiences. Scheduling these sessions was often difficult due to the competing demands of clinical rotations. The asynchronous components were viewed as more flexible but also described as repetitive and less engaging, limiting the impact on learning.
Theme Four: Value of the Biopsychosocial Model and Interpersonal Skills
Students highlighted the program’s biopsychosocial approach to interpersonal skills. Students reported that the LUI program reinforced the principles of patient-centered care and highlighted the relevance of the biopsychosocial model in clinical practice. Many felt the initiative supported their current understanding and expanded upon the importance of interpersonal skills in fostering effective therapeutic relationships and improving patient outcomes.
Theme Five: Engagement and Instructor Quality
Students emphasized the importance of instructor quality in shaping their engagement with the program. Students recognized and appreciated the LUI instructors’ enthusiasm and commitment, which contributed positively to the learning environment. However, they noted variability in the quality of discussions, with some sessions lacking consistency and personalized guidance, affecting the impact of the experience.
Theme Six: Impact on Clinical Practice and Future Career
Students offered their perspectives on how the LUI program influenced their clinical practice and shaped their views on future professional roles. Students varied in how they perceived the program’s impact on their clinical decision-making. Some felt LUI fostered valuable reflection and positively influenced their approach to patient care and future careers, while others reported minimal effect on their daily practice.
Discussion
This study examined the impact of a distance-based training program on the development of communication, empathy, and EI in second-year DPT students during their intermediate CEE, as well as the relationships among these competencies. Findings suggest that dedicated affective training is associated with increased levels of communication, empathy, and EI. Although interrelated, these constructs are distinct skills that require unique considerations and assessments. Additionally, students’ subjective experiences of the program help explain study findings and may inform future program development.
Findings further suggest that affective skills in DPT students are modifiable through targeted instruction. Following their intermediate CEE, only the experimental group showed significant improvements in communication, empathy, and EI, supporting the LUI program’s impact. Although these gains were relatively small, any positive shift is favorable given the previously documented decline in empathy and EI throughout DPT education.16,17,24
In contrast, the control group did not show any increases in the measures following their CEE. Although research suggests that EI can increase with cumulative clinical exposure,39 such gains are more commonly observed toward the end of DPT education and may be less evident during intermediate CEEs. This underscores the importance of incorporating structured affective training early in the clinical education sequence to accelerate growth in this area and reduce the prevalence of affective domain challenges across all CEE levels.5
Spiral Education
The spiral educational approach,40 an effective method for teaching healthcare students,41,42 helps contextualize these findings. This pedagogy emphasizes that skill mastery requires the revisiting of skills at increasing levels of complexity and depth. Affective skills such as empathy, communication, and EI are often introduced early in DPT education through foundational coursework and professional behavior expectations. However, students need to be challenged to refine and adapt these skills in new contexts, including high-stakes patient interactions, interprofessional communication, or complex ethical decision-making.
The LUI intervention performed concurrently with the students’ CEE may have reinforced this spiral process by intentionally situating affective training within more advanced and authentic clinical scenarios, thereby enabling learners to practice introduced concepts into richer, higher-order applications. This alignment with spiral learning principles may help explain why only the experimental group demonstrated significant increases in affective skills.
Group-level differences in age, race, program design, and content delivery may also have contributed to the differences in outcomes. Demographic and curricular variations were not controlled, as randomization to control or experimental groups was not feasible. Although the distribution of orthopedic versus non-orthopedic placements was similar between groups, variability in the quality of CEE, shaped by site characteristics, patient populations, and clinical instructor mentorship, may influence affective skill development. Prior research highlights the critical role of the clinical learning environment in shaping these outcomes,43,44 suggesting that placement variability may have moderated the observed effects.
A Novel Approach
The improvements observed in students who participated in the training program add to the growing evidence supporting strategies to enhance affective skills in DPT students.25,45 While contact hours were similar to previously studied interventions, the LUI program introduced a novel approach as it was delivered remotely and concurrently with students’ intermediate CEE, rather than embedded in the didactic curriculum.
For example, Goldsmith et al25 integrated a 10-hour empathy and communication module into a didactic course during the final month of a DPT program. Ross and Haidet45 delivered a 32-hour communication, mindfulness, and reflection course eight weeks before students’ first full-time CEE. Both studies showed gains in communication, confidence, and patient-centered behaviors. Compared to these in-person didactic-embedded models, the LUI’s hybrid format offered a flexible and scalable alternative that can be integrated directly into clinical education and supports virtual instruction as a practical adjunct to traditional classroom or simulated preparations.
Complementary Skillsets
We found moderate correlations among communication, empathy, and EI, as measured by the JSE, SSEIT, and SE-12 scales. These findings align with prior studies showing that individuals with higher levels of EI and empathy often demonstrate stronger communication skills.46-49 Due to this conceptual overlap, studies often use these affective constructs interchangeably.9,50,51 However, Quail et al52 demonstrated improvements in communication skills, knowledge, and confidence, exclusive of empathy skills, in speech pathology students after specific communication training. Consistent with the current study findings, this supports that these skillsets are complementary but distinct qualities. The LUI curriculum integrated communication and empathy training within a unified framework rather than through separate modules, yet deliberately attended to each construct individually. Therefore, it is reasonable to suggest that each construct requires specific attention in the assessment of students’ and clinicians’ abilities across educational, research, and clinical settings.
Informing Future Program Development
The focus group findings can help inform the development of future programs and curricular designs. Although compliance was relatively high, participants suggested that the training would be more effective if introduced earlier in the didactic curriculum or aligned with initial CEEs. Implementing affective skills training during early clinical exposures may ease students’ entry into clinical education, when affective challenges are most common.5 While the LUI curriculum was intentionally integrated with CEEs to facilitate immediate skill translation, students reported that concurrent delivery added to their workload and detracted from clinical learning. Given that clinical education is inherently stressful,24,53,54 students often prioritize CEE demands over LUI activities despite recognizing the program’s value. This is concerning, as underdeveloped patient-centered care skills are associated with greater burnout and reduced professional satisfaction.55
Delivering training with their initial CEE, when technical skill expectations are less rigorous, or during part-time integrated CEEs, may reduce burden while also bridging didactic instruction with authentic clinical application.
Participants underscored the importance of thoughtful delivery formats and content relevance. The LUI’s self-paced, hybrid model aligned with adult learning principles of autonomy and intrinsic motivation,56,57 yet many students perceived it as a checkbox task rather than an opportunity for growth. Despite measurable improvements in affective competencies, some noted redundancy of the LUI curriculum with their prior coursework. The increases may reflect the value of a spiral learning approach, which reinforces skills through repeated and increasingly complex applications.42 To strengthen engagement, future programs should explicitly communicate the intentional repetition.
The content delivery through an orthopedic lens contributed to difficulties sustaining student engagement and ensuring continuity for some participants. While the program aimed to create an energetic learning environment, some students, particularly those in non-orthopedic CEEs, struggled to connect with group discussion instructors and content. Since each clinical setting offers unique student challenges,5 the limited relevance for students in alternative clinical environments may have reduced opportunities for meaningful peer interaction and practical application. Expanding future training programs to include a broader range of clinical contexts would improve program effectiveness and promote greater engagement with the content across diverse CEEs.
Limitations
This study had several limitations. The differing response rates, age distributions, and lack of randomization between groups may introduce selection bias in the samples, affecting generalizability and the interpretation of results. Differences between the two DPT curricula may have influenced the outcomes; however, the authors attempted to control this potential confounder by ensuring that neither group participated in didactic coursework during the study period.
Although participation was voluntary and anonymous, the use of self-reported surveys introduces potential recall and social desirability biases that can affect external validity. Triangulating perspectives from patients, clinical instructors, or DPT faculty would have supported the accuracy of the self-reported measures to allow a broader applicability of the findings. Additionally, because the intervention was conducted at the authors’ institution, students may have been influenced by faculty presence or expectations. Study findings are limited to the LUI program, and extrapolating the effectiveness of alternative intervention approaches should be made cautiously. Despite efforts to ensure validity and reliability, only 10 students participated in the focus groups, which may not fully represent all perspectives. Although research indicates that analyses of two focus groups result in approximately 85% code saturation,58 full data saturation cannot be guaranteed, limiting the breadth and validity of the qualitative findings.
Suggestions for Future Research
Future research should explore and compare various approaches to developing interpersonal skills in DPT students. Examining the impact of targeted training during the CEE may offer valuable insight into how ongoing, experiential learning reinforces these skills.
Additional studies are needed to determine whether gains in affective competencies are maintained over time and influence clinical behaviors and patient outcomes post-graduation.
Lastly, future studies should consider how individual student characteristics and broader organizational culture influence interpersonal skills competency. A more comprehensive understanding of these factors can help refine educational strategies to ensure the delivery of high-quality, patient-centered care.
Conclusion
This study demonstrates the benefits of a distance training program in fostering communication, empathy, and EI among DPT students. These interrelated yet distinct skills can be effectively strengthened through distance and hybrid formats, providing a flexible, practice-oriented approach to learning. Affective qualities are essential to patient care and professional well-being, and educational models should continue to prioritize their development.
While challenges such as limited student engagement and organizational barriers exist, the findings emphasize the importance of integrating patient-centered skills into CEE and offer recommendations when developing future programs. Continuing to expand curricular strategies, refine delivery methods, and tailor content to varied clinical contexts may further enrich student learning.
Acknowledgments
The authors would like to acknowledge Zachary Gabor and Stephanie Allen for their coordination and delivery of the Level-Up Initiative, and Michael Masaracchio for assisting with control group recruitment.




