We are now in the midst of the age of brain research where innovative ideas and approaches offer exciting opportunities to unravel the complexities of the human brain. New technologies are evolving that provide unprecedented opportunities to study neuroanatomy. However, compelling visual displays are critically necessary to truly ‘see’ the brain. As the scientific community increases knowledge, a major challenge has become how to portray large volumes of complex information in a manner that is readily comprehensible by academicians and the general public alike. To meet this grand task, a renewed appreciation of the elements of visual design has emerged. Edward Tufte, a pioneer in the fields of visual design and data visualization, has underscored the power of the visual arts to convey complex and ground-breaking ideas, “To envision information—and what bright and splendid visions can result—is to work at the intersection of image, word, number, art.” 1 (p. 9)
The estimated total length of wires (axons of nerve cells) contained in the average young adult male human brain is 176,000km .2 Traveling this distance would take us nearly halfway from the Earth to the Moon. These wires are responsible for transmitting all information that makes us, well: ‘us’. It is now possible to use magnetic resonance imaging (MRI) as a way to non-invasively gather information detailing the structure and organization of these wires both in health and in the presence of disease.
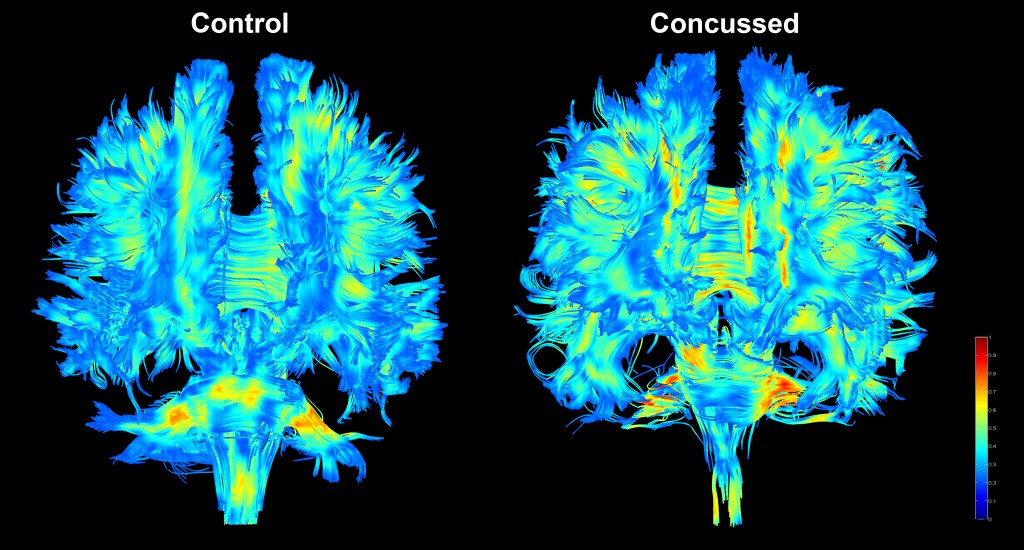
The accompanying image first appeared in Light Works – a free outdoor exhibit curated by the Royal Photographic Society to celebrate International Year of Light 2015 in four venues throughout the United Kingdom (http://www.rps.org/exhibitions-and-competitions/current-exhibitions/rps-light-works-exhibition/49). The image provides two visualizations of the structural architecture of the fiber pathways within the human brain. The information contained in these images was generated by applying a MRI technique known as diffusion tensor imaging, or DTI, to model brain fiber pathways after concussion.3 This technique is sensitive to the free movement of water (i.e. diffusion) that is directionally restricted by different brain tissue constituents (e.g. nerve axons). Using DTI, we can gain an understanding of the organization of pathways that are responsible for carrying all information to and from the brain as well as between different regions within the brain itself. Essentially using DTI, we are able to create an individualized wiring diagram for the brain of each patient.
In the images, the directionality of water diffusion is encoded by color where warmer hues represent greater directional preference for water diffusion and cooler hues indicate more random water diffusion. Thus, we are able to visualize aspects of the wiring throughout the brain using a single color-coded index. In the example provided, the tracts modeled in the brain of an adolescent after sustaining a concussion appear warmer than another adolescent that has not had a concussion which suggests there exists subtle pathology that could be a new target for therapeutic intervention. Not only does this approach provide a powerful visual of the structure of the brain, it also creates new information that enables a better understanding of injuries to the brain and how these injuries may impact human behavior.

This work is licensed under a Creative Commons Attribution 4.0 International License.