Purpose: Explore the perspectives of people with expertise on physiotherapy and/or Queer and Transgender (Trans) health regarding possibilities for transforming outpatient physiotherapy clinics to be inclusive of the Queer and Trans communities.
Methods: This research used a cross-sectional, descriptive, qualitative study design. Fifteen individuals with insight regarding cisgenderism and heterosexism in the context of Queer and Trans health, physiotherapy, and/or outpatient physiotherapy clinics in Canada completed one-on-one semi-structured interviews. Participants’ perspectives were organized into key themes through a thematic analysis approach following the DEPICT model.
Results/Discussion: Queer and Trans participants described strategies for transformative change in outpatient physiotherapy clinics at three levels. At the micro level, strategies involved individual clinics implementing changes to reduce Queer and Trans trauma and ‘labor’ as an initial step to meet the immediate need of Queer and Trans individuals within these spaces. At the meso level, participants emphasized that physiotherapists engage in learning and unlearning to build awareness of their own positionalities and Queer and Trans health needs. The macro level identified that community-led initiatives can push for large-scale policy and practice changes that disrupt and redistribute power from oppressors to Queer and Trans communities.
Conclusions: This study contributes to the understanding of how cisgenderism and heterosexism impact Queer and Trans patients and providers in physiotherapy and offers new insights and strategies into disrupting these two systems of inequality in outpatient physiotherapy clinics in Canada.
Key Words: Queer, Trans, physiotherapy, clinics, inclusivity, cisgenderism, heterosexism, 2SLGBTQIA+, cisnormativity, heteronormativity
Introduction
Systems of Inequality Impacting Queer and Trans Communities
Systems of inequality (eg, cisgenderism, heterosexism, colonialism, racism, ableism, classism), are historic and ongoing social structures that create unearned advantage for some, and oppression for others. One’s various social identities intersect to create interdependent arrangements of discrimination or disadvantage; the analysis of how systems of inequality produce these power imbalances is known as intersectionality.1–6 Cisgenderism and heterosexism are two intersecting systems that relate to sex and gender. These systems of inequality provide an unearned advantage (ie, privilege) to individuals who are cisgender and/or heterosexual, and an unearned disadvantage to individuals who are Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, and/or Asexual (2SLGBTQIA+), which we refer to in this article as Queer and Trans communities.4
Cisgenderism is an ideology that devalues people whose gender identity does not correspond with their sex assigned at birth.5 Heterosexism is an ideology that privileges being heterosexual.2–5 These two ideologies produce and are upheld by cisnormativity and heteronormativity, which are the beliefs that being cisgendered and heterosexual are the normal, right ways of being.7 These assumptions and beliefs are deeply ingrained and reflected in the way societal systems operate, including healthcare and education, as these are social determinants of health that contribute to health inequities.8–11
Cisgenderism and Heterosexism in the Context of Physiotherapy
In Canada, health disparities among Queer and Trans communities involve higher rates of cancer, chronic illness (including asthma, diabetes, and heart disease), and mental illness (including eating disorders, depression, and suicidal ideation/attempts).12 We posit that the source of these disparities are not biological but rather are socially, economically, and politically produced as a part of the systems of inequality described above. Queer, and especially Trans folks, experience increased violence and harassment in healthcare, greater barriers to accessing care, and thus lower rates of access to care.10,13–15 A 2019 report published by the Canadian House of Commons Standing Committee on Health (HESA) identified a lack of access to healthcare, and minority stress (additional stressors from the discrimination and stigmatization experienced by gender and sexual minorities), as primary contributing factors to poor health outcomes for people who are Queer and Trans.9
Barriers to accessing care included: stigma, discrimination or fear of discrimination, lack of knowledge by healthcare providers, and lack of tailored services.12 Ross and Setchell (2019) noted that many of the inequities described by the Queer and Trans patients in other healthcare settings are also pervasive in physiotherapy, including: implicit and explicit discrimination; fear of discrimination; normative assumptions of sexual and gender identities; and lack of knowledge on Transgender-specific health issues.10
A unique barrier to physiotherapy highlighted by this study is Queer and Trans patients’ discomfort related to bodily exposure, observation, and proximity, due to the physical nature of physiotherapy assessment and treatment.10 As a result of these barriers, Queer and Trans individuals are less likely to seek healthcare services, disclose pertinent health information, or receive appropriate healthcare services.12
Copti et al noted that healthcare professions, including physiotherapists, have neglected to acknowledge and include the cultural considerations and needs of Queer and Trans communities.16 Physiotherapists who themselves identify as Queer or Trans have identified pervasive cisnormative and heteronormative assumptions, including the burden of being viewed as less professional when failing to conform to cis/heteronormative patterns of behavior or self-expression portrayed through appearance, characteristics of relationships, and social lives outside of work.17 For example, those who did not “pass” as straight or cis based on their physical appearance, reported feeling exclusion, shame and frustration. A study by Ross, Hammond, and colleagues highlighted the physiotherapists’ experiences of ‘Queer labor’, which they define as emotional or other types of work that had to be done by physical therapists who are LGBTQIA+ to make their work environment safe and/or tolerable for themselves. This includes the work to hide aspects of their lives for safety, educate colleagues, and be a role model or advocate for the Queer and Trans communities.17
Systems-Level Changes to Address Inequities Faced by Queer and Trans Communities
Health disparities and inequities for Queer and Trans communities have resulted in a call for the physiotherapy profession to play a leadership role in bridging the gap.16 In 2019, the World Confederation for Physiotherapy (WCPT) released a statement outlining general recommendations to promote diversity and inclusion in marginalized populations, although not specific to the Queer and Trans communities.15 International physiotherapy bodies have recognized the need for best-practice guidelines to serve 2SLGBTQIA+ communities. These do not yet exist in Canada; however, there have been calls for a deeper understanding of current PT practice and education as it relates to 2SLGBTQIPA+ health.18–21
Engagement With Queer and Trans Communities
To produce transformative change, standards to improve health equity in physiotherapy settings must be co-created with Queer and Trans communities who are best positioned to disrupt cisnormativity and heteronormativity.10 However, there is a significant paucity of Queer- and Trans-informed literature to improve equity in physiotherapy settings.
Ross and colleagues offered recommendations from perspectives of Queer and Trans patients and physiotherapists to improve physiotherapy experiences in Australia.10,17,22 These included: learning and unlearning through LGBTIQ+ training for physiotherapists, health education specific to this population (especially for Transgender health), and the inclusion of gender diversity on forms to reduce Queer labor.10 This not only reduces the burden of work placed upon practitioners but the excessive work done by Queer and Trans patients to access healthcare.
Changes to better prioritize LGBTQ2S+ care in physiotherapy also include education and health policy at meso (institutional and organizational) and macro (societal) levels.11 Excitingly, research has shown that integration of awareness and training on the care needs of the Queer and Trans communities into the education curricula of physical therapy programs in the United States can improve physical therapy patient care.16 These studies offer preliminary ideas for implementing change; however, there is a lack of perspectives on experiences of physiotherapy in the Canadian context. Context-specific standards are key to driving transformative change, as unique impacts and opportunities may exist due to country-specific differences in physiotherapy-regulating bodies, healthcare, education, political systems, cultures, and histories of colonization.15
Therefore, the purpose of this study is to explore the perspectives of people with expertise on physiotherapy and/or Queer and Trans health regarding possibilities for transforming outpatient physiotherapy clinics in Canada to be inclusive of Queer and Trans communities.
Methods
Study Design
This research employed a qualitative, cross-sectional, descriptive study design. The study was informed by the critical perspective of the Coin Model of Privilege and Critical Allyship, such that it focused on how health inequities are shaped by intersecting systems of inequality that operate, in part, through fields such as physiotherapy.4 The inquiry was also informed by Rupa Marya’s Flowchart “Health and Justice: The Path of Liberation Through Medicine,” which outlines how different systems of oppression can lead to harm, trauma and poor health.23,24 This study was approved by the University of Toronto Research Ethics Board.
Positionality
The individual and intersecting social locations of the research team have influenced our experiences and worldviews, and therefore the assumptions we brought into this inquiry. The research team consisted of six graduate physiotherapy students (all identified as cisgender; one identified as Bi-curious, two as Bisexual, one as Gay, and two as straight) and three advisors (all identified as cisgender; two as Queer, and one as straight). All identified as white settlers in Canada. All identified as able-bodied, and three as neurodivergent. All advisors were employed, and students were unemployed, with no experience of poverty. Throughout the study, we sought to recognize and minimize the impact of our positions of privilege while centering expertise from embodied experiences of oppression.
Participant Inclusion/Exclusion Criteria
Inclusion criteria required participants to speak English, be at least 18 years old, and have expertise or insight regarding cisgenderism and heterosexism in the context of Queer and Trans health, physiotherapy, and/or outpatient physiotherapy clinics in Canada, which may include:
- Persons with expertise in how cisgenderism and heterosexism play out in healthcare (within and/or beyond physiotherapy) (eg, lived experience, advocates, researchers).
- Queer and Trans persons who are physiotherapists or other rehabilitation professionals.
- Queer and Trans persons working in private outpatient physiotherapy clinics, and especially clinic leaders.
- Queer and Trans persons who have sought private physiotherapy services at outpatient physiotherapy clinics.
We defined ‘having expertise or insight’ as self-reported experiential, embodied, academic, and/or other forms of knowledge that position individuals to assist us in addressing the research question.
Participants were excluded based on the following criteria to mitigate risk of coercion and power imbalances:
- Current students within the Department of Physical Therapy at the University of Toronto.
- Current patients of the clinical research advisors, or patients who had been discharged less than one year prior to the onset of the study.
We sought to recruit at least two participants from each inclusion criteria domain above (ie, a-d). Furthermore, we purposively sought participants with diverse sexual orientations and gender identities, and prioritized potential participants based on diverse social locations regarding ability, racialization, geographic location, and experience of poverty.
Sampling and Recruitment
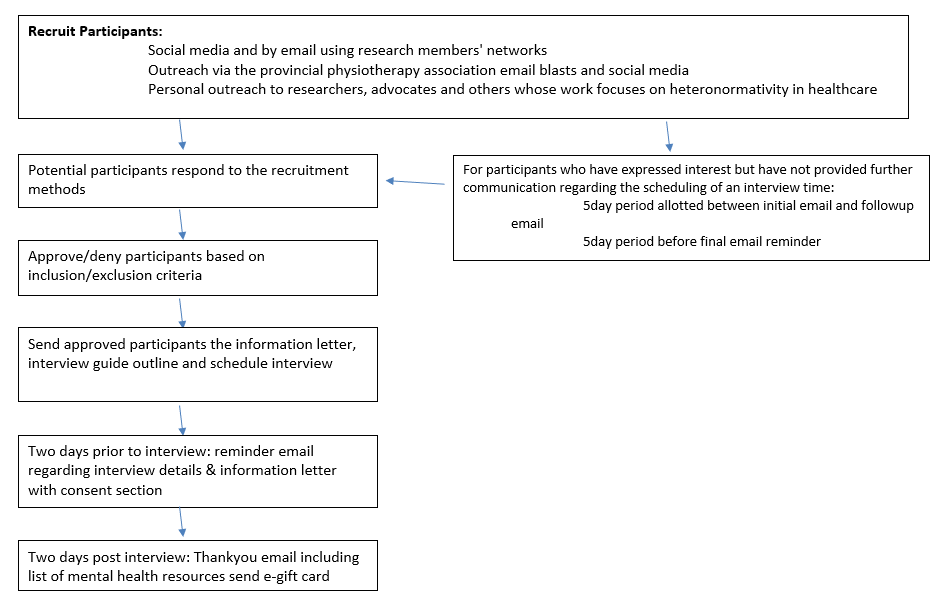
Participants were recruited from January to March 2022 via purposive sampling (Figure 1). Participants were offered a $25 e-gift card for their participation in the study. Team members sent recruitment emails to their personal and professional networks. Recruitment emails were also distributed to the Canadian Physiotherapy Association; provincial/territorial physiotherapy associations/branches; English-speaking research faculty within rehabilitation science departments at Canadian universities; research institutes; as well as Queer and Trans community and university-based organizations and advocates. E-flyers were distributed via social media through Instagram and Facebook accounts related to physiotherapy, rehabilitation, and Queer and Trans content. Individuals interested in participating contacted the research team via email; a team member then followed up to confirm their inclusion criteria and social locations. The research team sent a second and final wave of recruitment emails/social media blasts halfway through the interviewing process to elicit further participants and communicate a priority for interviewing underrepresented gender identities, sexual orientations, and other social locations to maximize diversity in the data.
Data Collection
In preparation for the data collection, three student researchers received guidance from the supervisors regarding how to conduct semi-structured interviews through three workshops. These workshops included watching example interviews conducted by the supervisors and piloting an interview with a supervisor. The student researchers then each piloted the interview guide twice among peers who fit some but not all of the inclusion criteria. Feedback from the pilot interviewees was taken into consideration for the final draft of the guide. Prior to starting the interviews, participants provided informed verbal consent.
One-on-one interviews were then conducted with each participant in a semi-structured format lasting 45 to 60 minutes over the Zoom video conferencing service and using a demographics questionnaire and interview guide. The guide consisted of open-ended questions regarding:
- How heterosexism and cisgenderism play out in physiotherapy clinics at the individual, interpersonal, and institutional level.
- Insights about the WCPT diversity statement.
- Perspectives on ways to improve inclusion of Queer and Trans communities in outpatient clinics in Canada.
The interviews were audio-recorded electronically via Zoom and transcribed verbatim by team members, then quality checked by the interviewer and a second student researcher to enhance rigor.25
Data Analysis
Data were collaboratively analyzed both inductively and deductively by all members of the research team through a thematic analysis informed by the six-step DEPICT model.26,27
In the first step, dynamic reading, as defined by the DEPICT model, transcripts were divided and independently reviewed by a minimum of two researchers to identify patterns within the data. In engaged codebook development, these patterns and other themes drawn from the literature and researcher experience informed the creation of a draft codebook.26,27 The codebook was independently pilot tested on transcripts by the student researchers. Results were compared in a collaborative meeting to identify revisions and finalize the codebook. The codebook was then utilized in participatory coding, whereby each transcript was independently coded twice. In the inclusive reviewing and summarizing of categories step, summaries of the data for each code were developed by one or two team members. Each summary was reviewed by another researcher and shared with the team during analysis meetings. During collaborative analysis, the research team reviewed the summaries and identified themes in the data.
These themes were further honed deductively through several iterations and consolidated into our final three data themes:
- Reducing Queer and Trans Trauma and Labor
- Learning and Unlearning
- Disrupting Systems of Power
The process of collaborative analysis and consolidating themes was done with input from existing frameworks in the literature, including the framework of ‘Survive, Dream and Build’ outlined by Zena Sharman in The Care We Dream Of and the frameworks previously mentioned in our study design.4,23,24,28,29 Zena Sharman’s work was brought in at this point as we felt it addressed a common point of tension throughout all the interviews between manageable immediate change and disruptive structural change. In the final step, translation, the research team drafted the manuscript text and a poster to describe the study results.
Results
Participants
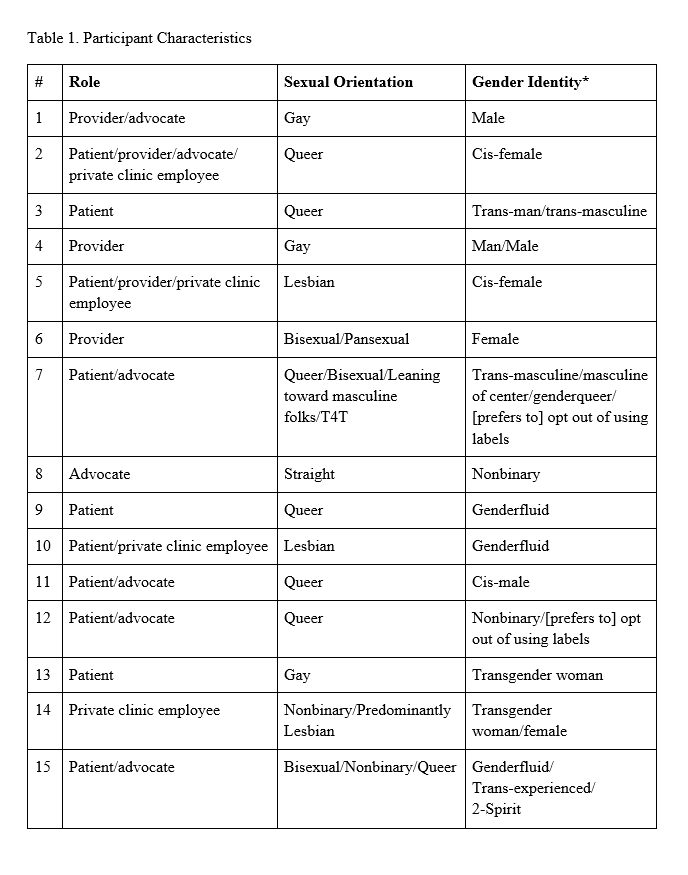
Fifteen participants were interviewed for this study, all of whom self-identified as being part of Queer and/or Trans communities (Table 1). Twelve participants self-identified as being white; others described their racial and/or ethnic identities as Nehiyaw/Cree, West Asian, Chinese, Tamil, and Filipino (noting that participants could identify with more than one identity). Two-thirds (n=10) of the participants resided in Ontario, four in British Columbia, three in Alberta, and two in Nova Scotia. Sixty percent of participants identified as able-bodied; others reported identities that included being neurodivergent (n=2), having chronic health issues (n=4), and being Mad (n=2). Forty percent of participants reported experience with poverty or not having their basic needs met. Thirteen of the 15 identified living in an urban setting, four identified suburban, and three identified as rural.
Themes
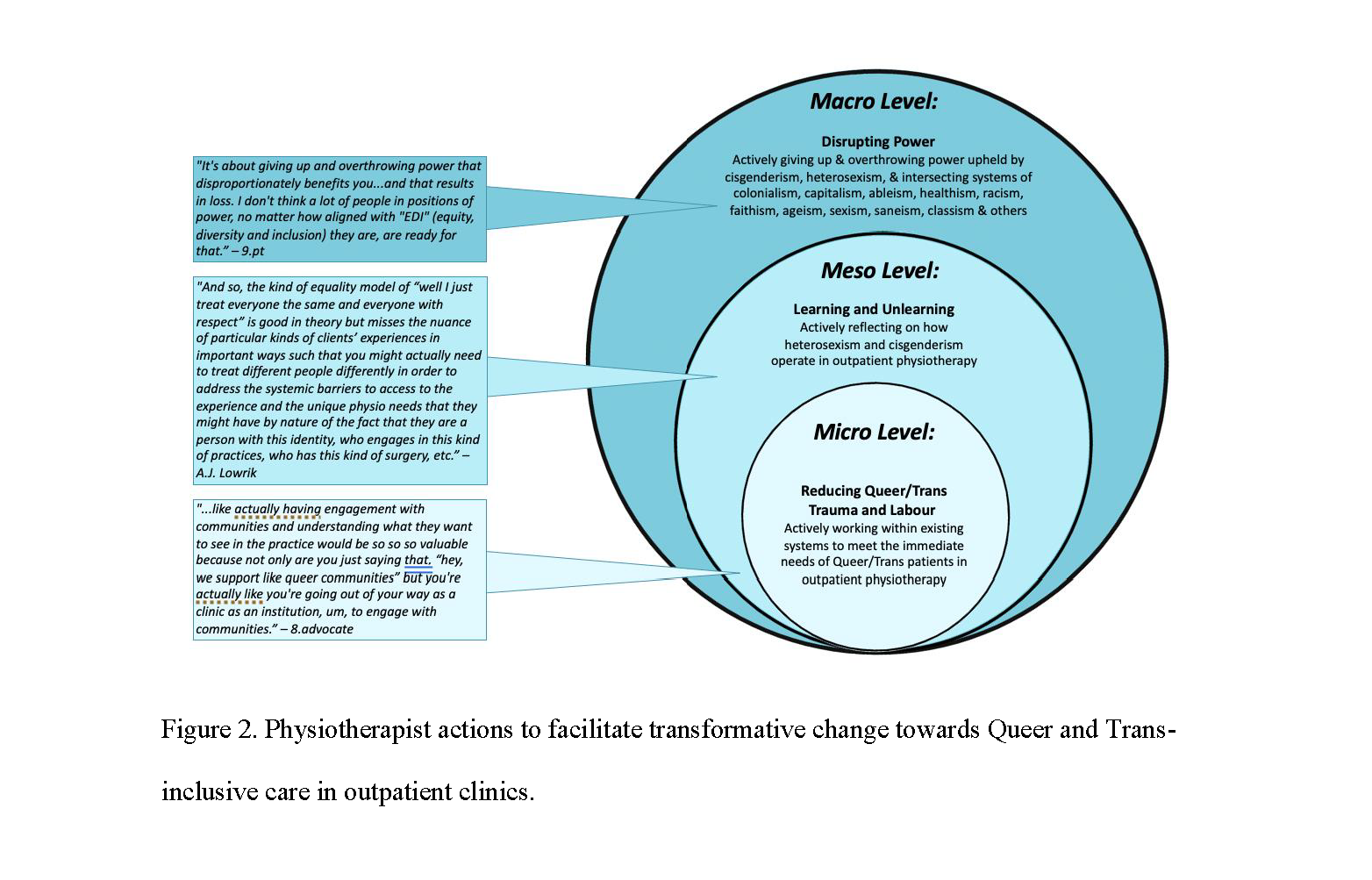
Participants described strategies for transformative change in outpatient physiotherapy clinics at three levels (Fig. 2).
- At the micro (individual) level, strategies involved individual clinics implementing changes to reduce Queer and Trans trauma and labor.
- At the meso (institutional) level, physiotherapists were called to engage in learning and unlearning that builds awareness of their own positionalities and Queer and Trans health needs.
- The macro (societal) level identified community-led initiatives that can push for large-scale policy and practice changes that disrupt power and redistribute that power from oppressors to Queer and Trans communities.
Micro Level: Reducing Queer and Trans Trauma and Labor
Participants shared that cisgenderism and heterosexism put an enormous burden on Queer and Trans people, and that immediate changes to outpatient physiotherapy clinics are required to meet Queer and Trans peoples’ needs. Patients and practitioners described emotional labor to cater to the emotionally fragile responses of cisgender and heterosexual peers when confronted with the need for interpersonal and institutional change. One practitioner relayed their interactions with colleagues:
“They are middle-aged white ladies who have a certain point of view and they really, really, really don’t like to be wrong. So, […] they just need some talking and coaching and persistence.” (Participant 2)
Both patients and practitioners noted putting effort into their clothing and behavior to outwardly conform to cisnormativity and heteronormativity. One nonbinary patient shared the work they put in to access safe pelvic floor physiotherapy (a specialized type of physiotherapy in which knowing a patient’s gender and/or sex may be necessary in order to provide appropriate care):
“When I do enter these highly gendered and sexed healthcare spaces, …I just kind of put my hair down. And I dress as femme as I can that day [laughs]. And I don’t correct people, and I don’t explain my identity… and I just am a chameleon in those spaces, because I don’t want to deal with inadequate or dangerous healthcare.” (Participant 9)
Participants reported that knowing which clinics had a good reputation for working with Queer and Trans people helped reduce the burden of masking their identity. However, Queer and Trans patients reported high levels of labor associated with seeking out Queer- and Trans-competent care, safe spaces for care or employment, or practitioners who would agree to treat them. One Trans participant described their experience of seeking post-surgical care for bottom surgery:
“Finding a pelvic physio for…post-surgical care…as a Trans woman was next to impossible. It took me upwards of six months… The one word that describes it would be exhausting.” (Participant 13)
Some patients reported that cisgenderism or heterosexism played less of a role in their physiotherapy access and treatment when they received care to “non-triggering” body parts that were unrelated to sex and/or gender, or they did not see their sexuality or gender as relevant to their physiotherapy care. Conversely, patients reported more labor and effort to conform to cisnormativity and/or heteronormativity in hiding aspects of their lives or access issues when receiving care for more “triggering” body parts, or areas of physiotherapy care that relate to sex and/or gender, including pelvic health and post-bottom-surgery rehabilitation.
In order to help Queer and Trans patients and practitioners locate culturally-safe clinics, multiple participants proposed the creation of a centralized database of Queer and Trans and allied physiotherapists, and suggested clinics display Queer- and Trans-friendly rainbow signage. Participants also recommended clinics to facilitate access to gender neutral washrooms, proactively record pronouns during the subjective assessment, provide gender diverse or neutral magazines/brochures in waiting areas, and be mindful of use of patients’ chosen names vs. legal names. A.J. Lowrik [participant requested that anonymity be removed for accreditation of their work], a consultant for businesses looking to improve their clinical spaces for Queer and Trans individuals, recommended that clinics simply “start somewhere” rather than waiting for a perfect implementation plan. Lowrik reported talking to a community member who said “…if I waited for gender-affirming care, I would never see a doctor ever again.”
Meso Level: Learning and Unlearning
Participants shared that to make meaningful change, practitioners must understand the ways in which the healthcare system fails Queer and Trans people. This includes physiotherapists learning about how their practice may perpetuate harm toward their patients. A prevalent message was that incessant cis- and heteronormative assumptions negatively influence the overall experience of healthcare.
“It’s when they [practitioners] hold those assumptions, […] and those ideals about like what they think my experiences are, or what they think my gender is, […] it communicates to me or it makes me see or realize that I don’t belong in this society, or I don’t belong in that clinic.” (Participant 8)
Participants stated that practitioners must unlearn their own assumptions and positionalities to better serve Queer and Trans patients.
“What it really takes is having…a very intentional unlearning […] I think that…education is really one of the most powerful ways to unlearn those habits and to learn more about perspectives that you just perhaps would never be exposed to otherwise.” (Participant 5)
Participants reported that physiotherapists should “… take your lead from the patient” (Participant 3), when discussing gender or sexuality so that care remains relevant to the patient, and irrelevant questions are not asked purely out of curiosity from the practitioner.
Participants reported that cisnormativity and heteronormativity are also prevalent in the healthcare education system. One participant described a lack of Queer and Trans representation within physiotherapy educational leadership positions while another participant (a current student in a healthcare field) reported being ‘called out’ by a professor who told him that he did not present as Queer:
“A professor said to me the other day, ‘You know, you don’t present as a Queer person.’ Like I was so surprised. And so then there was an effeminate guy over there, and I said, ‘Yeah, well, what do you think about that guy over there?’ ’Oh, yeah, yeah, I do think he’s Queer.’” (Participant 11)
The majority of participants in this study agreed that healthcare students, practitioners, and others in patient-facing and policy-making roles should be educated on cisgenderism and heterosexism, a critical history of Queer and Trans people, critical reflexivity in communication strategies, harm-reduction strategies, gender-affirming language, and trauma-informed care. It was stated that this specialized type of focused education is required to appropriately work with this population.
“… I think that there almost needs to be some form of education […] that there are going to be differences (in patients)… and you need to be aware of that, because if you’re not, that person very frequently will stop seeking help’.” (Participant 7)
Some participants even suggested that this education should be a mandatory requirement for licensing:
“… all practitioners need to have a certain number of hours of mentorship or continued education in order to renew their licenses every year […] that system is already in place […] So why not, just, you know, toss inclusivity and intersectionality courses into that education?” (Participant 10)
Participants also strongly emphasized that education or the development of training workshops should be informed by individuals who hold that lived experience:
“… when you’re creating programs or when you’re trying to have a discussion about these topics.[…] You should probably speak to someone within that community beforehand.” (Participant 6)
A few participants reiterated that delivering trauma-informed care is particularly relevant for Queer and Trans participants whose relationship with their own body might be impacted by the trauma of cisgenderism and heterosexism. One participant, a nonbinary healthcare student, described the way in which they perceived the education system shapes healthcare providers’ relationship with the human body to be “…entitled and transactional in nature” (Participant 11). They explained the importance of ongoing consent and intention during both assessment and treatment, encouraging a practice in which “…touch is not just touch, but it’s touch to care as well.” (Participant 9). They explained that the touching required on behalf of the healthcare provider serves a greater purpose than assessment and treatment, and further provides care for the whole of the patient.
Macro Level: Disrupting Power
The participants of this study reported several opportunities for dismantling oppression toward Queer and/or Trans individuals. These included but were not limited to provincial or national policy/legislature, and capitalism (profit driven economic systems) within the Canadian education and healthcare system. Participants suggested more radical changes were needed to dismantle interlocking systems of oppression, which requires redistribution of power and community-led health.
Participants provided numerous specific examples of how profit-based models of care are detrimental to Queer and Trans health. Participants described how clinic owners prioritized profit over the health and wellbeing of both patients and staff; for example, not allowing patients additional time to communicate gender-affirming language to use:
“I just found that there was so much pressure within a private practice clinic because they’re, […] trying to sort of get you to see as many people as possible, […] and sometimes that subjective piece or just building rapport gets pushed aside.” (Participant 4)
Multiple Queer and Trans patients described their experiences of not being able to afford outpatient physiotherapy, with one nonbinary participant reporting:
“…people going into private clinics is like taking away from the social welfare aspect of things […] because Queer folks are disproportionately poor.” (Participant 8)
This participant further provided suggestions on how to target this inequity:
“…that should be addressed at the policy level. […] at least as an intermediate step, subsidize cost, […] especially […] if there are […] long lines, […] for the public sector.” (Participant 8)
Another participant further commented on the benefits of socializing physiotherapy, to include it under the universal healthcare system, to improve both regulation and access for all:
“If physiotherapy were socialized […] there are regionally recognized policies that places must abide by. […] I can only think that that would be better.” (Participant 13)
Multiple participants emphasized increasing the number of Queer and Trans physiotherapists trained and hired, as they have the potential to deliver quality care as well as advocate for change within their profession:
“Ultimately, the best way to serve these communities is to have these communities represented among your staff.” (Participant 12).
However, participants acknowledged the social capital required to be accepted into physiotherapy school, and that Queer and Trans applicants face extensive oppression even when they are admitted to the program. One gender Queer participant noted:
“…think of how […] exclusionary and oppressive the Academy is, even if acceptance criteria changes…I think the conversation tends to end […] once we have X Y Z seats filled with marginalized people […] It doesn’t take into consideration how going into this program, […] will negatively affect them [laughs].” (Participant 9)
Another suggested mechanism of collective action was to directly target regulatory and state policy. One participant noted this type of change could be achieved through a Charter challenge of the Canadian Charter of Rights and Freedoms (whereby individuals in Canada can challenge a court to strike down government actions or laws if they believe their rights or freedoms are being violated) 30 :
“…changes to the governing body can come from charter challenges. […] that’s the hammer that makes it happen.” (Participant 13).
Overall, many participants felt that individual clinic changes alone would not lead to transformative change in physiotherapy. One participant pointed out that clinics are often not willing to make larger changes to a system that benefits them:
“It’s about giving up and overthrowing power that disproportionately benefits you…and that results in loss. I don’t think a lot of people in positions of power, no matter how aligned with quote, EDI, they are, are ready for that.” (Participant 9)
A Two-Spirit participant rooted our understandings of outpatient physiotherapy clinics in a Canadian history of settler colonialism as well as white and Christian supremacy. They emphasized the importance of engaging in emotional, physical, mental and spiritual LandBack (the reclamation of everything stolen from Indigenous peoples) to decolonize physiotherapy:
“…that’s what LandBack is,[…]. It’s an actual physical, spiritual, emotional and mental process. […] you’re actively seeking right relation with local, regional, and national Indigenous, you have good relations, and you maintain them.” (Participant 15)
This participant also reinforced the necessity for caring for all beings and the land when engaging in physiotherapy:
“…limitations are colonial in nature. Indigeneity never believed in being limited. So, all streams reach the ocean, not just the convenient one […] colonial philosophy is […] all about competition. So, it doesn’t matter if you’re disabled, Trans, or poor, or homeless, or drug-addicted, right? […] The very things we do to the land, in the air, in the water, through our willing obliviousness. But that’s how the system is built. …we do the same thing to ourselves.” (Participant 15)
True Queer- and Trans-competent care thus involves caring for all aspects of health, and all persons, not just those that are convenient or easy. Overall, participants emphasized the importance of putting words into action and warned against clinics including Queer- and Trans-inclusive symbols if they were not prepared to follow through with Queer- and Trans-competent care. Participant 1 described this as follows:
“…it’s kind of […] living what you preach, […] there’s a lot of clinics who have their diversity statement because they know they should have it, but I don’t know if their day-to-day operations reflect that.”
Discussion
This study sought to identify Queer and Trans perspectives to guide transformational change for equitable care in outpatient physiotherapy clinic services in Canada. To our knowledge, this is the first study to gain such insights pertaining to physiotherapy outpatient clinics in Canada. This study highlights opportunities for promoting Queer and Trans health equity among individual physiotherapists and physiotherapy organizations.
Micro Level: Reducing Queer and Trans Trauma and Labor
This study’s findings of participants’ experiences of ‘labor,’ or additional required effort to overcome cisnormative and heteronormative standards in physiotherapy, are consistent with findings from both patient (Ross 2019, Ross 2023) and provider (Ross 2022) perspectives in other studies.10,17,31 These studies also similarly highlighted the participants’ emotional and physical labor required to mask themselves as cis/heteronormative in order to avoid discrimination and feel safe, or additional effort to educate others and act as a role model.
Our findings further reinforce previously well-established “manageable actions,” or micro-level recommendations, in the literature to facilitate access to and treatment within physiotherapy in order to reduce Queer and Trans trauma, such as changes to physical environments and intake forms.10,13,17,18 The findings overall urge outpatient physiotherapy clinics and individual physiotherapists to expand supportive spaces to prevent Queer and Trans patients from feeling the need to mask their identity, hide aspects of their lives that may be pertinent to their care, or avoid seeking physiotherapy altogether.
A novel finding of our study is the report of additional labor required for Queer and Trans patients accessing physiotherapy for which sex and gender may be emphasized, such as pelvic floor physiotherapy. Participants reported labor in seeking out rehabilitation for gender-affirming surgeries (eg, top surgery and bottom surgery) and post-surgical rehabilitation. As such, physiotherapists and other healthcare providers must take greater responsibility for changing practices in which cis- and/or heteronormativity is more pervasive in order to mitigate the additional burden placed on these patients.31
Suggestions include providing a referral to the appropriate care that affirms patient identities and does not pathologize differences in gender identity or expression. Physiotherapists should consider a trauma-based approach, by offering privacy and clarifying ongoing consent for touch during physical therapy assessment, and not assume gender based on body parts (eg, prostate cancer, postpartum care).32,33
In identifying the excessive Queer and Trans labor required to work within and access the healthcare system, participants highlighted the urgent need for allies and community members to take initiative immediately and not just wait for systemic-level changes to kick-in. While all participants acknowledged that systemic change was necessary, many emphasized that they needed care now and thus highlighted accessible ways for allies and community members to engage in mutual aid and critical allyship, which increases access to physiotherapy for Queer and Trans patients and practitioners.
In Zena Sharman’s The Care We Dream Of: Liberatory Approaches to LGBTQ+ Health, she outlines a pathway to transformative change in healthcare that necessarily includes practices that enable the survival of the Queer and Trans community.28,29 This then creates the space needed for creativity, imagination, and the purposeful practice of dreaming a different healthcare system. Leah Lakshmi Piepzna-Samarasinha expands on what this accessible care looks like in a description of ‘crip healing,’ which takes the lead from the historical knowledge of Queer and Trans disabled community members and includes anything that helps someone’s disabled body/mind.34,35 Our participants’ reflections reinforced these ideas—that it is alongside the care measures of survival that we can begin to dream and build radically-inclusive physiotherapy clinics.
Meso Level: Learning and Unlearning
Participants’ experiences of assumptions regarding their gender and sexual orientation impacting their healthcare experience is consistent with the current literature regarding Queer and Trans perspectives in the physiotherapy profession, in other health professions, and more broadly throughout society.10,17,22 Findings in all studies consistently report that patients and health workers assume that actors in the health system are straight and fit into a gender binary. These assumptions thus shape the physical space and culture.10,17,22
For example, intake forms include only male or female classifications, or partners are assumed to be heteronormative.10,17,22 This is where Nixon’s Coin Model of Privilege and Critical Allyship can assist us in understanding the difference between intention and impact. For instance, we can assume that physiotherapists are well intentioned and do not seek to harm, exclude, or marginalize Queer and Trans patients or staff. Yet by being unaware of the ways intersecting systems of oppression operate through our actions (eg, how we frame our intake forms), physiotherapists unwittingly reproduce and uphold the intersecting coins of cisgenderism and heteronormativity.4
Participants’ emphasis on education as a method to combat cisnormative and heteronormative assumptions also aligns with findings from studies executed among physical therapy education in the United States, as well as with other healthcare professions.10,13,17,18,36 A study in the United Kingdom found that students with exposure to the Queer and Trans communities had fewer cisnormative and heteronormative beliefs, and more inclusive attitudes.36 Hence, exposure and education for physiotherapists may be impactful for reinforcing the unlearning of cis and heteronormative beliefs.
Participants in this study recommended increased Queer and Trans content in the physiotherapy curriculum, with opportunities to learn directly from Queer and Trans individuals, which is consistent with previous research and recommendations regarding strategies to challenge pervasive cisnormativity and heteronormativity.10,17,31 Small-group role-play and case vignettes were effective in encouraging physical therapy students in the United States to provide more Queer- and Trans-competent care.16 This learning format could serve as a model for ways in which Canadian physiotherapy programs can incorporate more education and exposure specific to Queer- and Trans-competent care as role-playing, and how case vignettes are already widely used throughout curricula. However, compensation to Queer and Trans persons is necessary to offset the labor put into education.
Macro Level: Disrupting Systems of Power
Participants’ linking of cisgenderism and heterosexism in physiotherapy to settler colonialism, white supremacy, and Christian supremacy is a novel finding within this study. Other healthcare professions in Canada, including the Nursing Association of Ontario, have also acknowledged that binary concepts of gender and sexuality are products of colonization, rooted in Euro-Christian and Westernized dominant systems of belief.19 Further, research by Rupa Marya has outlined how trauma, inflammation, and poor health outcomes are directly reproduced by interlocking systems of supremacism, colonization, and capitalism in the medical context.23 However, this is the first study to our knowledge to provide explicit suggestions to dismantle broader systems of oppression; for example, by socializing physiotherapy, promoting the education of more Queer and Trans physiotherapists, changing policies and legislation regulating physiotherapy and healthcare bodies, and ultimately decolonizing Canadian healthcare.
Further research is lacking on the impact of capitalism (including for-profit healthcare) on conditions of Queer and Trans persons within outpatient physiotherapy clinics. However, Israel et al (2008) found that a number of therapy professions in the United States lacked awareness of the broader impact of funding and agency structures on marginalized access to care.37 Another study found that Trans patients in the United States did not seek healthcare due to financial barriers.38
Similar to findings in Ross et al in 2022, we found that profit-driven models of care in private outpatient physiotherapy clinics lead to rushed and therefore inadequate care.17 In addition, costs and a scarcity of rural-based locations are often barriers to Queer and Trans patients.17,39 Physiotherapists may be pressured to forgo providing extra time or effort in providing resources for Queer and Trans patients due to either managerial or personal pressure to be profitable and see as many patients per day as possible.
A McMaster study of 2SLGBTQIA+ workers in Sudbury and Windsor, Canada found that Queer and Trans workers are overrepresented in precarious work and felt pressure to remain in poor work conditions where staff happened to be supportive.40 Novel findings from our study suggest that Queer and Trans physiotherapists may feel the need to placate homophobic or transphobic clientele or colleagues in a more senior position due to financial implications. For example, Queer and Trans physiotherapists working through commission may feel pressured to conform to cisgender and heterosexual norms. They may also ignore cisgendered and heterosexist actions/comments from patients and those in more senior positions at their workplace to prevent losing clientele or job opportunities.
Participants also warned clinics against ‘pinkwashing’ or ‘rainbow-washing’, which is the use of Queer and Trans symbols as marketing tools for profit or credibility without materially addressing the needs of Queer and Trans communities or meaningfully dismantling structural oppression.41,42 This is consistent with criticism of platforming corporations in Canadian Pride events, some of whom have historically and presently engaged in colonial and supremacist violence against Queer and Trans Communities, especially those who are Indigenous, Black, or racialized.43–47
However, there is little research to our knowledge examining pinkwashing within healthcare or physiotherapy spaces. Novel findings from our study examine the tension between taking micro insider/institutional steps to Queer and Trans inclusivity in physiotherapy (as described above in ‘Reducing Queer and Trans Labor’) and engaging in radical disruptive change involving or led by extra-institutional community groups. Duplan (2023) examines this tension in interviews with Queer and Trans feminist municipal public officials who in some instances were able to prioritize the needs and perspectives of Queer and Trans community collectives over those of the institution.48 However, a ‘representation’ model of institutional change was challenged by some of the participants in our study who cited that Trans people in particular are only 1% of the population and thus could never be represented in every physiotherapy clinic.49 Ultimately, participants emphasized the importance of working within and without institutions on both micro and macro levels simultaneously.
The Native Youth Sexual Health Network (2016), a group who advocates for increasing access to identity-affirming support through culturally-safe sexuality and reproductive health rights, suggests the need for public health and community service providers to restore Indigenous knowledge systems, ceremonies, and ways of living as a way to reduce the power imbalance and harm of colonial practices in education and health.50 Our findings align with these recommendations, with some participants suggesting a need for decolonizing care from the influence of Euro-Christian and Westernized practice norms, especially while interacting with the Indigenous Two-Spirit, Queer and Trans communities.
Finally, participants suggested collective activism as a mechanism of change, which is consistent with a strong history of advocacy, activism, and mutual aid within the Queer and Trans community on Turtle Island (North America).50–52 Some participants emphasized the importance of redistributing power to achieve transformative change in physiotherapy, which is a core tenet of many Queer and Trans organizing groups. For example, the AIDS Coalition to Unleash Power (ACT UP), an activist group that worked to demand action to address the AIDS crisis, emphasized that in order to effectively disrupt power, resisting change must be more costly to decision makers than giving in.53 Many more community groups have organized in Canada to address increasing waves of Queer and Trans hate and push for transformational change in healthcare and other social systems.54–56 While there are health-provider or physiotherapy-partnered community advocacy groups, physiotherapists should participate in community-led activism to support Queer and Trans healthcare specifically, including legislative change.11,57,58 Taking bold action is urgently needed as violence against Queer and Trans communities is on the rise.59,60
Limitations
This was an exploratory inquiry involving 15 participants. As such, many perspectives are not reflected in these results. For instance, we note that a majority of participants were white, thereby limiting embodied experience of how systems such as white supremacy can interact with and reinforce cisgenderism and heterosexism. Importantly, the limited participation of Indigenous and Two-Spirit voices restricted our insights into physiotherapy that is Queer- and Trans-competent and decolonizes care (eg, LandBack). Although discussed, this paper did not deeply explore the nuances of the relationships between disability, white supremacy, and religion with cisgenderism and heterosexism within a rehabilitation context. We also did not capture the voices of Queer and Trans caregivers, who may face additional labor when accessing the healthcare system on behalf of their families. Finally, we would like to emphasize that the depth of the inquiry in this study is further limited by the fact that all members of the research team are cisgender and white. Thus, the research team lacked representation from important perspectives such as the Trans community or People of Color.
Future Directions
Future research should further explore the richness and diversity of perspectives on how to create transformative change for Queer and Trans people in healthcare, including the perspectives of Queer and Trans caregivers and of Queer and Trans members who were not directly given voices in this study. Perspectives of Two-Spirit persons and other Indigenous members of the Queer and Trans community should be recruited due to the unique intersection of colonization with this population. Additionally, it would be of benefit to identify further perspectives on the nuanced intersectionality of other systems of oppression, including white supremacy and disability, in their relationship to cisgenderism and heterosexism.
Further research should also focus on implementation of Queer- and Trans-specific best practices into outpatient physiotherapy clinics and education. Finally, future work should explore other physiotherapy settings, such as publicly-funded outpatient clinics, hospitals, and homecare, as well as across different health professions.
Conclusion
In this study, we centered on those with insight regarding cisgenderism and heterosexism in the context of Queer and Trans health, physiotherapy, and/or outpatient physiotherapy clinics in Canada. This allowed for a unique examination of the ways in which physiotherapists can recognize and disrupt the impact of cisgenderism and heterosexism on their patients and colleagues and the physiotherapy profession. This study builds on previous literature on the impacts of cisgenderism and heterosexism by further illuminating nuances of these systems of oppression, including increased trauma and labor for both Queer and Trans patients and physiotherapists, specifically within the outpatient clinic setting.
We offered a conceptual framework highlighting these findings with three specific recommended levels of change (micro, meso, and macro) that physiotherapists can implement into their professional practice in a necessary, collective effort to be more inclusive of the Queer and Trans communities within their clinical spaces. The framework highlighted the importance for physiotherapists to:
- Reduce Queer and Trans trauma and labour.
- Recognize and interrupt their assumptions of cis- and heteronormativity through learning and unlearning.
- Dismantle cisgenderism and heterosexism through redistribution of power to the Queer and Trans communities through policy and government-level changes.
Acknowledgements
This research was completed in partial fulfillment of the requirements for a Master of Science PT degree at the University of Toronto. We express appreciation to the participants who graciously shared their time and expertise; this study would not be possible without their contributions. We acknowledge the research unit coordinators, Dr. Kelly O’Brien, Dr. Esther Waugh, Dr. Crystal MacKay, and Dr. Darlene Reid, for their guidance. Finally, we thank Michelle Legasto-Mulvale and Stephanie Scodras for their patience and assistance.
Acknowledgement of financial support: Honoraria for participants was provided by Lindsay Beavers through her 2021 Temerty Award for Excellence in Professional Values.
Acknowledgement of conflict of interest: We have no conflicts of interest to declare.
Glossary
*Definitions may vary and the particular definitions detailed here may not perfectly reflect the experiences or identities of participants
| Term | Definition |
| 2-Spirit/Two-spirit | Two-Spirit, a translation of the Anishinaabemowin term niizh manidoowag, refers to a person who embodies both a masculine and feminine spirit. The concept of two-spirit was first introduced by Elder Myra Laramee. Activist Albert McLeod helped develop the term in 1990 to broadly reference Indigenous peoples in the lesbian, gay, bisexual, transgender and queer (LGBTQ) community. Two-spirit is used by some Indigenous peoples to describe their gender, sexual and spiritual identity. |
| 2SLGBTQIA+ | An acronym which stands for 2-spirit, Lesbian, Gay, Bisexual, Trans, Queer, Intersex, Asexual and more. |
| AIDS | Acquired Immune Deficiency Syndrome |
| Bi-curious | Someone who considers themselves heterosexual but has a sexual or romantic ‘curiosity’ toward the same gender |
| Bisexual | Romantic or sexual attraction or behavior toward more than one gender or to both people of the same gender and different genders. |
| Bottom surgery | A type of gender confirmation surgery in which a person’s genitalia are altered to align with their gender identity. Generally refers to vaginoplasty, phalloplasty or metoidioplasty |
| Capitalism | An economic and political system in which a country’s trade and industry are controlled by private owners for profit |
| Cis/cisgender | Denoting or relating to a person whose gender identity corresponds with the sex registered for them at birth; not transgender |
| Cisgenderism | Cisgenderism refers to the system of oppression that gives unearned advantage (privilege) to people who are cisgender, and unearned disadvantage (oppression) to people who are not. |
| Cisnormativity | Cisnormativity is the assumption that everyone is, or ought to be, cisgender. The term can further refer to a wider range of presumptions about gender assignment, such as the presumption of a gender binary, or expectations of conformity to gender roles. |
| Colonization | The action or process of settling among and establishing control over the Indigenous people of an area. |
| Consent | Permission for something to happen or agreement to do something. Consent should be ongoing. |
| Decolonization | The undoing of colonialism, returning power and sovereignty to Indigenous peoples. |
| Gay | Sexually or romantically attracted exclusively to people of one’s own sex or gender (used especially of a man) |
| Gender | Gender includes the social, psychological, cultural and behavioral aspects of being a man, woman, or other gender identity. |
| Gender-Affirming Care | Gender-affirming care encompasses a range of social, psychological, behavioral, and medical interventions “designed to support and affirm an individual’s gender identity” when it conflicts with the gender they were assigned at birth. |
| Genderfluid | Denoting or relating to a person who does not identify as having a single unchanging gender |
| Genderqueer | Denoting or relating to a person whose gender identity does not correspond to conventional binary gender distinctions |
| Heteronormativity | Heteronormativity is the assumption that everyone is, or ought to be, straight. It is the idea that romantic and sexual relationships are always between one man and one woman. Heteronormativity assumes heterosexuality is the default sexual orientation, and the only normal or natural way to express sexuality and attraction. |
| Heterosexism | The system of oppression created by the assumption that heterosexuality is the one, normal, correct sexual orientation; this system produces unearned advantage (privilege) for people who identify as heterosexual or “straight” and unearned disadvantage (oppression) for people who do not. |
| Heterosexual/straight | People who are heterosexual, or “straight,” typically feel sexual and romantic attraction toward people who are of a gender different than their own. |
| LandBack | Land Back, also referred to with hashtag #LandBack, is a decentralised campaign by Indigenous Australians, Indigenous peoples in Canada, Native Americans in the United States, other indigenous peoples, and allies alike, that seeks to reestablish Indigenous sovereignty, with political and economic control of their ancestral lands. In other words the physical, mental, spiritual and emotional reclamation of everything stolen from Indigenous peoples by colonizers. |
| Lesbian | Typically a woman or non-binary person who is sexually and/or romantically attracted to other women or non-binary persons. |
| Mad | Mad is a reclaimed word by people who may identify as mad, mentally ill, psychiatric survivors, consumers, service users, patients, neurodivergent, and disabled. Mad-positive pedagogies often center on ways Mad persons’ experiences represent sites of/for learning holding deep knowledge and value. |
Neurodivergent/ Neurodiversity | Neurodiversity is a framework for understanding human brain function and mental illness, which views diversity in human cognition as normal and whereby some conditions classified as mental disorders are differences that are not necessarily pathological. |
| Nonbinary | Denoting, having, or relating to a gender identity that does not conform to traditional binary beliefs about gender, which indicate that all individuals are exclusively either male or female. |
| Oppression | Unfair and unjust treatment of or exercise of power over, a group of individuals that is received not based on worth or behaviour but because one finds oneself in a social group designed to be disadvantaged by a historic system of oppression; includes exclusion, dehumanization and forms of violence that predictably produce inequities |
| Pansexual | Sexually or romantically attracted to people regardless of their sex or gender |
| Privilege | A special right, advantage, or immunity granted or available only to a particular person or group. Unearned advantage that is received not based on merit or behaviour but because one finds oneself in a social group designed to benefit from a historic system of oppression. |
| Queer | Denoting or relating to a sexual or gender identity that does not correspond to established ideas of sexuality and gender, especially heterosexual and cisgender norms |
| Top surgery | Surgery to alter the appearance of one’s chest to align with their gender identity. |
| Trans/Transgender | Denoting or relating to a person whose gender identity does not correspond with the sex registered for them at birth. |
| Trans man | A trans man (short for transgender man) is a man who was assigned female at birth. Trans men have a male gender identity, and some trans men undergo medical and social transition to alter their appearance in a way that aligns with their gender identity or alleviates gender dysphoria. |
| Trans masculine | Transmasculine, sometimes abbreviated to transmasc, is an umbrella term that describes a transgender person (generally, but not exclusively, one who was assigned female at birth), and whose gender is masculine and/or who express themselves in a masculine way. |
| Trans woman | A trans woman (short for transgender woman) is a woman who was assigned male at birth. Trans women have a female gender identity, and some trans women undergo medical and social transition to alter their appearance in a way that aligns with their gender identity or alleviates gender dysphoria. |
| Trans 4 Trans (T4T) | Transgender people may experience sexual and romantic attraction to other transgender people. This attraction is sometimes called T4T (“trans for trans”). |
| Trauma-informed care | Trauma-informed care is a framework for human service delivery that is based on knowledge and understanding of how trauma affects people’s lives, their service needs and service usage |
| Turtle Island | Turtle Island is a name for Earth or North America, used by some Indigenous peoples, as well as by some Indigenous rights activists. |







